I. Introduction
Health information exchange (HIE), defined as the reliable and interoperable electronic sharing of clinical information among providers and patients across the boundaries of healthcare institutions and other entities, is an integral component of the health information technology infrastructure [12]. The technology is expected to improve the speed, quality, safety, and cost of patient care by enabling care providers to access patients' care information across various organizations at the point of care [345]. Countries facing the problems of escalating healthcare costs and falling healthcare quality see this technology as one of viable solutions to improve the effectiveness and efficiency of their healthcare systems, and they are making efforts to adopt and diffuse the technology through various strategies with varying degrees of success [6789].
Efforts to introduce the technology have been unsuccessful in South Korea (hereafter, Korea), although the need for HIE infrastructure is greater than any other countries whose healthcare delivery system is highly fragmented, while care at different providers are disconnected. HIE was successfully piloted in Korea with government funding during a 3-year period (2007–2010) from patient referrals between a tertiary care hospital and local clinics [1011]. However, further attempts have not been made to extend or expand the pilot project since its completion in 2010. Another pilot project started in 2015 with the identical setting to the previous one, but differing in the participation of multiple tertiary hospitals without a clear plan for expansion in terms of the scope and scale of the project [12]. Previous studies have reported numerous challenges to be overcome for successful implementation that is sustainable and capable of realizing the expected benefits of the technology. These challenges include coordinating the interests of stakeholders, such as providers, insurers, patients, regulators, and policy makers; reassuring the public regarding their concerns about information safety and security; and securing funding to build and operate an interoperable, safe, and secure HIE [13]. Recent studies have emphasized the importance of government financial and regulatory support among those challenges, and government support is possible when there is public support for the cause [1415]. Public acceptance and sentiment toward the technology remains a significant challenge to the successful implementation of the infrastructure as information technology profoundly changes society.
Most studies on the public acceptance of HIE have reported public agreement with the need for the technology, which stems from the belief that HIE would improve the quality of medical care and increase patient convenience and satisfaction [16171819]. Studies have also reported that concerns about information privacy and security discourage the use of HIE [172021]. The factors reported to influence public acceptance can be categorized into two groups: personal characteristics and system characteristics. Personal characteristics include age, gender, income, health status, and experience with HIE [16171819]. System characteristics include the types of health information to be exchanged and the types of recipients [2223].
The objectives of this study were two-fold: to assess the public acceptance of HIE and to identify factors influencing public acceptance. We used the Technology Acceptance Model (TAM) proposed by Davis et al. [24] to investigate the study objectives, which posited that an individual's perceived usefulness (PU) and perceived ease of use (PEOU) of information technology influence his/her attitude toward using it, and behavioral intention to use is affected by PU and attitude, and actual system use is affected by the intention. We surveyed a representative sample of the general public in Korea who were 19 years and older to obtain data to be used in the analyses. The study results are expected to contribute to the formulation of a strategy and policy for HIE rollout in Korea and in other countries who are experiencing difficulties in introducing the technology infrastructure in the era of public resentment over misuse and security breaches of sensitive private information.
II. Methods
1. Conceptual Model
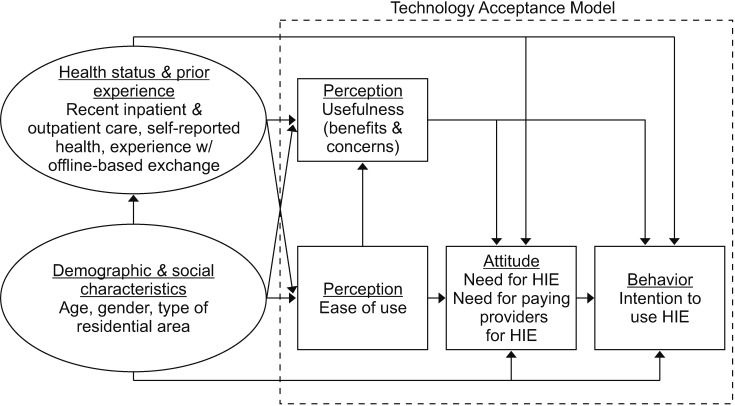
We modified the TAM proposed by Davis et al. [24] to examine the study questions as presented in Figure 1. Figure 1 shows the influence of PEOU on PU and attitude towards HIE, the influence of PU on attitude and behavior, and the influence of attitude on behavior towards HIE.
We included two groups of variables, demographic and social characteristics and health status and prior experience with offline-based information exchange, such as a paper copy of medical records or diagnostic imaging files stored on a CD or memory stick, as control variables in the model. We assumed that health status and experience with offline-based information exchange would affect all components of TAM and that the demographic and social characteristics of individuals would affect all components of TAM as well as health status and experience with offline-based information exchange.
2. Data
We constructed a structured survey instrument to obtain data to be used in the assignment of numerical values to the constructs of the conceptual model presented in Figure 1. The questionnaire consisted of four parts: (i) demographic and social characteristics, (ii) health status and prior experience with offline-based information exchange, (iii) PEOU and PU (benefits and concerns) of HIE, and (iv) attitude and intention to use HIE. We included 3 questions regarding age, gender, and type of residential area (metropolitan, city, and rural); 3 questions regarding health status (recent experience with outpatient and inpatient care, and self-reported health status on a 5-point Likert scale); 1 question regarding experience with offline-based information exchange; 1 question regarding PEOU; 13 questions regarding PU of HIE; 2 questions regarding attitude (need for HIE and incentive payment to providers for the provision of HIE measured on a 5-point Likert scale), and 1 question regarding the intention to use HIE. Three questions used to assess the health status are from the Korea National Health and Nutrition Examination Survey [25].
We used the questionnaire developed and used by Park et al. [19] in the third part of the survey, which was designed to assess patients' PU with multiple-item scales. HIE is expected to improve the quality and efficiency of care delivery. Park et al. [19] operationalized the quality of care with five attributes (expedited care process, improved diagnosis accuracy, improved doctor-patient communication, improved provider-patient relations, and patient convenience by reducing the burden involved with information exchange), and measured the attributes with multiple-item scales. They also measured the efficiency of care benefit of HIE with multipleitem scales. We included eight questions regarding the five attributes of the quality benefit, three questions regarding the efficiency benefit, and two questions regarding concerns. The extent of interviewees' responses were measured on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). We pre-tested the survey instrument with about 20 potential interviewees to assess the clarity of wording and time to complete the survey.
We surveyed a population of individuals 19 years or older selected by stratified random sampling with proportional allocation using population statistics based on resident registration in June 2017 [26]. The strata were defined by age, gender, and administrative residential region. Residential regions were stratified further by the type of residential area, which classified the address into three categories: metropolitan, city, and rural. We hired a public opinion research firm in Korea, which had a good reputation for high-quality surveys for the sampling and data collection. Thirty trained interviewers performed telephone interviews through random digit dialing that was built by the firm for telephone surveys during the period between August 11 and 22, 2017.
3. Analytical Methods
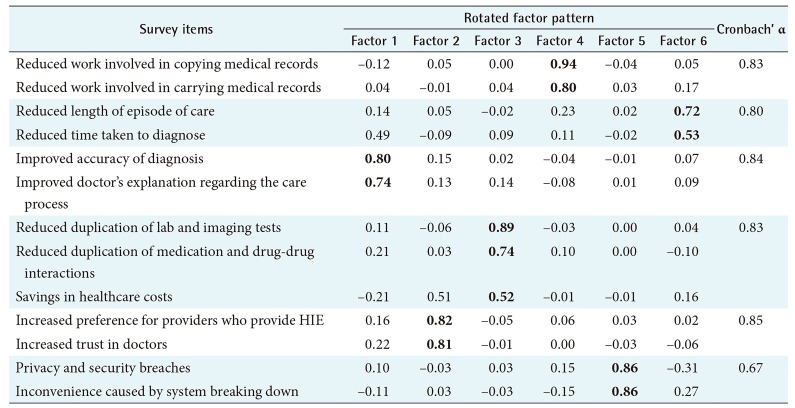
We assessed the validity and reliability of the 13 survey questions used to measure respondents' PU of HIE with exploratory factor analysis and Cronbach's alpha coefficients. We used principal factor analysis to extract factors with squared multiple correlations as prior communality estimates. We pre-rotated factors by the orthogonal varimax method. Then, the final rotation was conducted by the oblique promax method.
We computed frequency distributions of demographic and social variables, health status, and prior experience with offline-based information exchange to gain an overview of the general characteristics of the study sample. We computed descriptive statistics for responses measured on a 5-point Likert scale and frequency distributions for categorical responses to assess the constructs of TAM: PEOU and PU (benefits and concerns) of HIE, attitude towards HIE, and intention of using HIE.
We used a Structural Equation Model (SEM) to estimate the magnitude and significance of influences among the constructs of the conceptual model. The assumed distributions of endogenous variables in the analysis were:
- (0, 1) binary scale for recent experience with inpatient and outpatient care; experience with offline-based information exchange; and intention of using HIE (yes or no response),
- ordinal scale for self-reported health status; PEOU; attitude towards the needs for HIE and paying providers for the provision of HIE, which were based on a 5-point Likert scale to record responses,
- continuous scale for six attributes of PU of HIE, which were computed using the 13 questions which were recorded on a 5-point Likert scale.
We executed logistic regression for the binary and ordinal scale endogenous variables and generalized least square (GLS) regression for the continuous endogenous variables. We estimated the percentage of increase in the odds for category one above as the value of the independent variable increases by one with all other variables held at a fixed value using a coefficient estimate obtained from the logistic regression as in Equation (1): where β ^  is coefficient estimate.
is coefficient estimate.
is coefficient estimate.We used the statistical software package STATA/SE 13.1 (StataCorp LLC, College Station, TX, USA) for statistical computation and tests.
III. Results
1. The Characteristics of the Sample and the Validity and Reliability of the Survey Instrument
The general characteristics of the study sample are presented in Table 1. The age distribution and the type of residential area distribution approximately reflected the distributions of the population [26]. Fifty-five percent of the study sample had experience with offline-based health information exchange, such as carrying hardcopies of medical records and diagnostic images stored on a compact disk or USB drive.
The results of the analyses executed to examine the validity and internal consistency of the survey instrument are presented in Table 2. The exploratory factor analysis grouped 13 questions included in the questionnaire to assess the PU of HIE into six factors, which represented the attributes of benefits and concerns of HIE. There were five factors for benefits-improvement in diagnosis accuracy and doctors' communication regarding care processes, improvement in provider-patient relations, decrease in duplication of care and healthcare costs, convenience of HIE by reducing the burden related to health information exchange, and expedited care process. There was one factor for concerns, namely, privacy breaches and system break down. All factor loadings were over 0.5, and Kaiser's measure of sampling adequacy (MSA) was 0.91, which indicated that the analysis results fit well. Cronbach's alpha coefficients, which reflect how well a group of items asked differently for an attribute focuses on the attribute consistently, were mostly over 0.70, which is used as a threshold for acceptable values. We defined six variables to measure the attributes of PU of HIE based on the analysis results.
2. Public Acceptance of HIE
Descriptive statistics of responses to the questions included in the survey to assess the constructs of TAM are presented in Table 3. The average level of agreement regarding the ease of use of HIE technology was 3.2, which is a little higher than the neutral level. The average levels of agreement for the questions concerning benefits of HIE ranged from 3.76 to 4.49. Respondents agreed most highly with the statements that HIE would reduce the burden of copying and carrying medical records, which is an intrinsic function of HIE (4.49 and 4.38). The next highest agreement was found for the statements that HIE would expedite care processes by reducing the time required for diagnosis (4.32 and 4.30). Then, the statements regarding the reduction of duplicated medication and adverse drug interactions and the reduction of duplicated tests followed (4.29 and 4.25). The levels of agreement concerning the benefits of improved doctor-patient communication, reduction of healthcare costs, and improved diagnosis accuracy were lower in comparison to other benefits (4.0, 3.99, and 3.95). The statements for which there was least agreement were about provider-patient relations with averages of 3.84 and 3.76. The levels of agreement with the statements concerning adverse effects of the technology were between the levels of ‘neutral’ and ‘agree’ (3.69 and 3.46).
The respondents' acceptance of the technology was high. The average level of agreement with the need for HIE was 4.16, and 87% of the respondents expressed their intention to use HIE. However, the respondents were not enthusiastic about paying providers for provision of the service. The average was 3.04 which is right at the neutral level.
3. Factors Influencing Public Acceptance
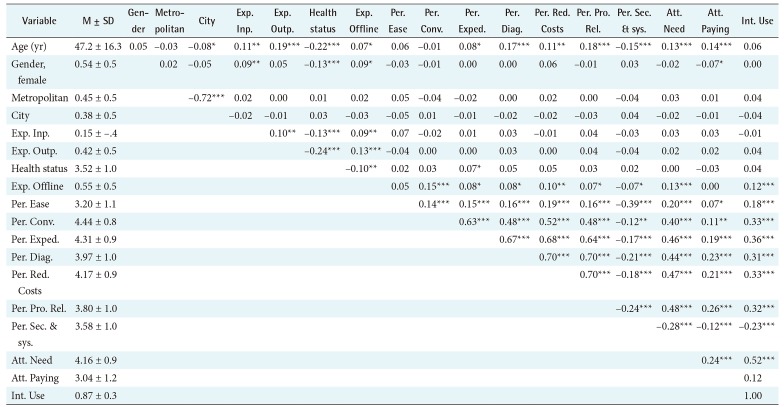
Descriptive statistics and Pearson correlation coefficients between variables are presented in Table 4. Age was correlated with most variables in the model with varying degrees of significance except for the intention to use HIE, PEOU, and the convenience benefit. Experience with offline-based information exchange was significantly correlated mostly with perception, attitude, and intention variables except for the PEOU and the attitude about paying providers for HIE. The perception, attitude, and intention variables were positively correlated with each other with a high degree of significance except for the perception of the concern about the technology, which showed significant negative correlations.
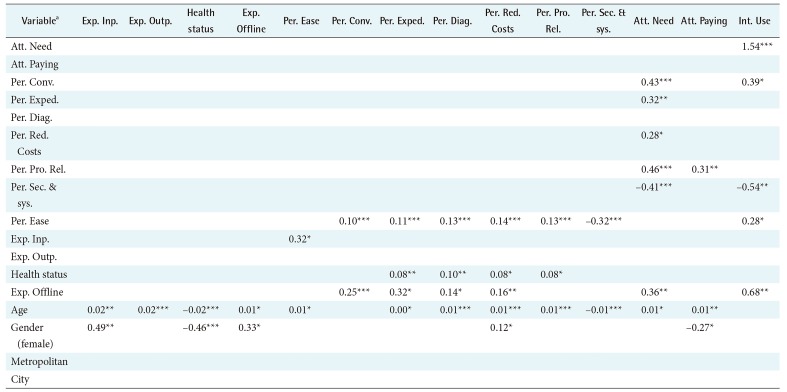
Coefficient estimates of SEM are presented in Table 5. The log-likelihood of the fitted model, the Akaike information criterion (AIC), and the Bayesian information criterion (BIC) were −15,062, 30,440, and 31,210, respectively.
The variable with the largest positive influence on the intention to use HIE was the attitude towards the need for the technology (coefficient estimate = 1.54, p < 0.0001). The results indicate that the odds for choosing to use HIE increased by 366% as the level of agreement with the statement regarding the need increased by one when all other variables were held at a fixed value. The variable with the second largest influence was prior experience with offline-based information exchange. The odds of choosing to use the technology for respondents with such experience were 97% higher than those without such experience (p < 0.01). Perception about the convenience benefit of the technology had a positive direct influence on the intention to use (coefficient estimate = 0.39, p < 0.05) and a positive indirect influence through the influence on the attitude towards the need for the technology. The PEOU of the technology had a positive direct influence on the intention to use (coefficient estimate = 0.28, p < 0.05) and had positive indirect influences through the positive influences on perceptions of convenience, expedited care process, reduced care duplications and costs, and improved provider-patient relations benefits. The perception about the concerns of information security and system reliability negatively influenced the intention to use (coefficient estimate = −0.54, p < 0.01). The odds of choosing to use HIE decreased by 42% as the value of the variable increased by one with all other variables held at a fixed value.
The attitude towards the need for HIE was directly positively influenced by the perception of technology benefits: convenience (0.43, p < 0.0001), expedited care process (0.32, p < 0.01), reduced duplication of care and costs (0.28, p < 0.05), and improved provider-patient relations (0.46, p < 0.001). It was negatively influenced by the perception of technology concern: security breaches and system break down (−0.41, p < 0.0001). Also prior experience with offline-based information exchange and age influenced attitude positively (0.36, p < 0.01 and 0.01, p < 0.05, respectively). However, attitude was not directly influenced by the PEOU; rather, it was indirectly influenced by the PEOU through the perception of benefits and concerns of the technology. Variables with a direct positive influence on the positive attitude towards paying providers for the service provision were the perception of provider-patient relations benefit and age (0.31, p < 0.01 and 0.01, p < 0.01, respectively). Also, female respondents were less likely to agree with paying providers for HIE (−0.27, p < 0.05).
All attributes of PU of HIE were significantly influenced by the PEOU of the technology as TAM posited. The directions of the influences of benefits were positive, whereas the perception of concerns had a negative influence. As the level of agreement with the statement regarding the PEOU of HIE increased by one, the levels of agreement with the statements regarding convenience, expedited care process, improvement in diagnosis and communication, reduced duplication of care and healthcare costs, and improvement of provider-patient relations increased by 0.1, 0.11, 0.13, 0.14, and 0.13, respectively (all significant at p < 0.0001). The level of agreement with the statement regarding information security and system reliability concerns deceased by 0.32 (p < 0.0001) as the level of agreement with the statement regarding PEOU increased by one. Self-reported health status, prior experience with offline-based information exchange, and age also directly influenced the PU of HIE. Respondents' concern about information safety and system reliability decreased as age increased (−0.01, p < 0.0001). Respondents who had inpatient care in the previous year had a higher level of agreement with the statement about PEOU (0.32, p < 0.0001), and age influenced PEOU positively (0.01, p < 0.05).
Age directly and indirectly influenced the constructs of TAM: perceptions, attitudes, and intention. Age was also significantly associated with the control variables that we included in the model to measure health status and previous experience with offline-based information exchange. The probability of having inpatient care in the previous year increased by 1.85% (p < 0.01), having outpatient care in the past two weeks increased by 2.51% (p < 0.0001), having self-reported health status decreased by one level increased by 2.36% (p < 0.0001), and having offline-based information exchange increased by 0.87% (p < 0.01) as age increased by one and all other variables were held at a fixed value. The probability of having inpatient care in the previous year for female respondents was 63.55% higher than for male respondents (p < 0.01). Female respondents' odds of selfreported health status increasing by one level (direction for better health) was 36.57% smaller than for male respondents (p < 0.0001) and having offline-based information exchange was 39.32% larger (p < 0.05). The type of residential area did not influence any of the variables in the model.
IV. Discussion
This study attempted to assess the public acceptance of HIE and to identify factors influencing public acceptance in an effort to draw implications in the policy formulation for wider adoption of HIE. We built a conceptual model based on TAM and used data from a survey of 1,000 individuals whose age and type of residential area distributions were similar to the distributions of the population to assign numerical values to the model constructs. We found that the respondents' level of acceptance of the technology was quite high, and their perceptions of benefits surpassed their perceptions of concerns. The acceptance of an aged population and a population with prior experience with offline-based information exchange was particularly high, which largely confirms the study results reported by Park et al. [19], although the study was conducted in a different setting. However, respondents' attitude towards paying providers for providing HIE was neutral, although an aged population and a population with high expectations for the benefit of provider-patient relations improvement showed a higher interest in comparison to other segments of respondents. Therefore, the public is highly in favor of the technology, but is not in favor of paying for it.
The results confirmed the influences proposed by TAM [24]. First, individuals who have a higher level of PEOU of HIE have higher levels of perceptions of benefits of the technology and lower levels of concerns. Second, higher levels of perceptions of benefits lead to a positive attitude about the need for it, and individual with these perceptions and attitudes are more likely have the intention to use the technology [2728]. Third, higher levels of concerns lead to a negative attitude and lower likelihood of having the intention to use it [2728]. Fourth, the likelihood of individuals having the intention to use the technology increases as individuals' attitude toward the need for HIE strengthens.
Age and prior experience with offline-based information exchange were the two most influential control variables, which showed a wide range of influences throughout the model. Respondents expressed high expectations for convenience benefits, and this perception had the greatest impact on the intention to use the technology when direct and indirect impacts are combined. However, their expectation for the healthcare cost savings benefit was low and the impact was weaker in comparison to the impacts of other benefits.
We draw three implications from the study findings for implementing policies and strategies for wider adoption of HIE. First, the study results imply that persuading the public to fund providers' investment in HIE infrastructure would be a formidable task for policy makers despite the high public acceptance, which has been identified as an important factor for sustainable implementation of the technology by previous studies [1314]. The study results showed that attitude was directly and indirectly influenced by age, indirectly by health status and recent experience with inpatient care, indirectly by the PEOU of the technology, and directly by the perception of technology benefit for improving provider-patient relations. Policy makers need to collect evidence of technology benefits and to communicate the evidence with those who are young and healthy. Second, age was a significant confounding factor that had an influence on the variables throughout the model. This finding indicates the importance of a tailored implementation strategy for groups of population segmented by age. Third, respondents' perception about the adverse effects of the technology, such as information privacy breaches and system unreliability, was a significant indicator of the low acceptance of HIE, although the level was ‘neutral’. The variables that directly and indirectly influenced the perception negatively were age, recent experience with inpatient care, and the PEOU of the technology. Administrators of the system should be extra careful not to have any adverse events in the first place, to invest in technology and education for attaining and maintaining the capability needed to achieve a high level of system security and reliability, and to maintain active communication with the public on the issue.
This study is not free from limitations. First, most of the survey participants did not have experience of actually using HIE, which is the limitation of most studies of new technology acceptance. However, the study results confirmed most of the findings of Park et al. [19], which analyzed data from a survey of patients who had experienced the technology. Second, one of TAM constructs, PEOU, was measured with a single survey item in this study and the validity and reliability of the measurement could not be assessed. Lastly, a variety of diagnostic statistics of the SEM, such as rootmeansquare error of approximation (RMSEA), goodness of fit index (GFI), normed-fit index (NFI), comparative fit index (CFI), Tucker-Lewis index (TLI), standardized rootmean-square residual (SRMR), and chi-square could not be assed in this study because our SEM included mixed types of endogenous variables and the statistical software package we used, STATA/SE, does not compute diagnostic statistics other than AIC and BIC for SEM models with mixed types of endogenous variables. However, we checked that the AIC and BIC of our model were better than those of SEM with assumptions of all continuous endogenous variables. Despite these limitations, the results of this study should provide policy makers with valuable information and evidence of need for the technology in the face of opposition to the technology rollout.