Adoption of Electronic Health Records: A Roadmap for India
Article information
Abstract
Objectives
The objective of the study was to create a roadmap for the adoption of Electronic Health Record (EHR) in India based an analysis of the strategies of other countries and national scenarios of ICT use in India.
Methods
The strategies for adoption of EHR in other countries were analyzed to find the crucial steps taken. Apart from reports collected from stakeholders in the country, the study relied on the experience of the author in handling several e-health projects.
Results
It was found that there are four major areas where the countries considered have made substantial efforts: ICT infrastructure, Policy & regulations, Standards & interoperability, and Research, development & education. A set of crucial activities were identified in each area. Based on the analysis, a roadmap is suggested. It includes the creation of a secure health network; health information exchange; and the use of open-source software, a national health policy, privacy laws, an agency for health IT standards, R&D, human resource development, etc.
Conclusions
Although some steps have been initiated, several new steps need to be taken up for the successful adoption of EHR. It requires a coordinated effort from all the stakeholders.
I. Introduction
The current status of the healthcare sector in India is associated with low public spending (1% of GDP), high out-ofpocket payments (71%), a high level of anemia among young women (56%), high infant mortality (47/1,000 live births), and high maternal mortality (212/100,000 live births), etc. The country lags behind other countries, such as Bangladesh and Sri Lanka, when it comes to the health of its people. The situation is worse for the poor as they cannot afford healthcare at high rates from private sector providers, which currently serve 78% of outpatients and 60% of inpatients [1].
According to the working paper (series 1) of the Health Division of the National Institution for Transforming India (NITI) Aayog [2], the infant mortality rate (IMR) and under 5 mortality rate (U-5MR) have declined during the last two decades, but the rate of decline is lower than those of neighboring countries, such as Bangladesh, Nepal, Cambodia, among others. Similarly, the maternal mortality rate (MMR) has declined, but it is lower than those in Nepal, Vietnam, and other countries. The Human Development Index in the country has grown by 1 unit only since 2008, whereas it has grown by 4 in Nepal and 2 in Bangladesh since that time.
This highlights the need for major reforms in the healthcare sector. Though information and communication technology (ICT) cannot work as a panacea, it can provide a cost-effective solution to improve the quality and coverage as demonstrated in other countries. The last two decades have witnessed a series of national e-health initiatives launched by developed countries and several developing countries to harness the advances in ICT to improve the quality of healthcare and bring down its cost [3]. According to the US International Trade Administration's Health IT Top Markets Report [4], the estimated global healthcare expenditure during 2015 was more than US$ 7 trillion, and it is likely to exceed US$ 9 trillion by 2020. The global IT market was US$ 1.36 trillion in 2015, and it is likely to reach US$ 1.7 trillion by 2020. Most countries are in the process of reform in the healthcare sector, and use of IT is a key component of the process.
The objective of the present study was to develop a roadmap for India for the adoption of Electronic Health Record (EHR) systems. India has seen the benefits of ICT in transforming the lives of its people by the use of ICT in banking, railway reservations, public service delivery, etc. The same can be achieved in the healthcare sector too. The proliferation of mobile phones and the availability of high-speed Internet offer the possibilities to provide healthcare services in rural and remote areas of the country.
II. Methods
Two sources of information were used—the reports available in this area and experience in the implementation of ICT solutions in the country. The documents/reports reviewed included those from various concerned government agencies, such as the Ministry of Electronics & IT and the Ministry of Health & Family Welfare, and NITI Ayog (the erstwhile Planning Commission of India). We also reviewed reports on strategies for the adoption of EHR in other countries, e.g., Canada, Germany, the United States. Some reports published by organizations such as the Healthcare Information and Management Systems Society (HIMSS) were also included. The countries were selected based on the level of successful implementation of EHR systems across the country. We included two types of countries, those that have a national health system, like the UK, and those that have largely industry-driven healthcare facilities, like the United States.
The second source of information used was experience in the implementation of various IT projects in the healthcare sector over a period of more than a decade. The author has been involved in the conceptualization and implementation of several ICT projects in the healthcare sector, including Electronic Medical Record (EMR) for oncology, technology for EHR exchange, libraries for standards, telemedicine networks, and personal health record management system, etc. The author has also worked on several national-level committees constituted by Ministry of Electronics & IT [5] and Ministry of Health & Family Welfare [6] to steer the activities related to the development and deployment of ICT solutions in the healthcare sector.
The reports of several countries on EHR implementation were analyzed to find what types of activities have been initiated for EHR adoption. It was found that the activities can be grouped along four major dimensions. These are ICT infrastructure creation, Policy & regulations, Standards & interoperability, and Research, development & education. The information on the present situation of ICT solutions and infrastructure in the country was used to decide how the activities could be applied in India. Though the activities recommended are on the same pattern, the implementation suggested takes care of the local situation. For example, the use of open-source software is quite important in India though it may not be so important in other countries.
III. Results
To formulate a strategy for the implementation of EHR systems in India, it is necessary to look into these initiatives to benefit from their experience. In the following two subsections, we briefly discuss the status of EHR adoption in several countries and that in India.
1. International Scenario
Canada launched an initiative in 2001 to modernize its ICT infrastructure in healthcare [7]. In 2015, EHRs were created for 91% of Canadians, and 91,000 clinicians were using EHR systems in their work. The number was 62,000 in 2014; thus, there was significant growth. Further, 77% of family doctors were using EHR, which is three times the percentage in 2007.
In 2001, England started a national initiative called the "National Plan for IT" (NPfIT) for modernizing its healthcare system [89]. Under the initiative, Summary Health Records (SCRs) were created for 54 million persons (96% of the population).
In Germany, about 90% of physicians in private practice are using EHR systems. Patient privacy has been given adequate attention in the initiative. The patient can decide to hide or block any entry in the health record [10].
New Zealand has achieved an EHR adoption rate of 97%. At present, there is no central or single EHR system, but a distributed EHR system, which can be accessed from any entity across the nation. The country is aiming to have a single EHR system by mid-2018 [11].
In Korea, most tertiary hospitals have started using EHRs. A nationwide health information exchange (HIE) platform is being built for the exchange of health information among the healthcare facilities. The platform supports open application program interfaces (APIs) to implement a document registry, a document repository, and a master patient index. They use various standards, such as HL7, CDA, and Integrating the Healthcare Enterprise (IHE) Cross-enterprise Document Sharing-b (XDS.b) profile to build a nationwide secure HIE [12].
The United States has been working on the adoption of EHR for quite some time [13]. The federal government is providing financial incentive to those who make 'meaningful use' of EHR [14]. The incentive is given through the Office of National Coordinator (ONC) for Health Information Technology to those who have started using EMRs [15]. According to the data available, in 2014, 76% of hospitals had adopted basic EHR systems. It has been reported that 97% of the acute care hospitals have adopted certified EHR systems.
2. National Scenario
India has a mixed system of healthcare consisting of a large number of hospitals run by the Central Government and State Government as well as the private sector. In general, the level of use of ICT in the healthcare sector in the country has been lower in comparison to other countries. At the same time, both union and State Governments are working on several fronts to make use of the opportunities offered by ICT. Private sector hospitals are also in the process of implementing ICT projects, including electronic patient records.
Some of the corporate hospitals in India, such as Max Health, Apollo, Sankara Nethralaya, Fortis, etc., have implemented integrated ICT systems in place, covering all aspects, i.e., registration and billing as well as laboratory and clinical data. Max Healthcare hospitals started implantation of EHR in its hospitals in 2009 and achieved Stage 6 level of the EMR Adoption Model, which is used by the HIMSS for assessment of the level of adoption of EMR systems in any hospital [16]. Max Healthcare Group received the recognition for two of its hospitals—East Wing, Saket and West Wing, Saket, New Delhi in 2012.
The Apollo Group also has implemented EHR in its hospitals and achieved Stage 6 in the EMR Adoption Model for four of its hospitals located at Chennai, Nandanam, Aynambakkam, and Jubilee Hills [17].
Sankara Nethralaya (SN) has implemented an EMR system in its hospitals and satellite clinics in Chennai [18]. It engaged Tata Consultancy Services (TCS) for the implementation. SN and TCS also offer the EMR suite and hospital management system to other hospitals.
However, even in private hospitals, EMRs are rarely exchanged between hospitals. These remain in the same hospital and are referenced when the patient visits again. There is no authentic report on the number of patients whose EMRs/EHRs have been stored so far.
3. Analysis
As mentioned above, the reports of several countries were analyzed to find the activities that have been crucial parts of their strategies. Regarding infrastructure, it was observed that there are several areas in which governments are investing. These include the creation of ICT infrastructure in healthcare facilities, secure health information communication networks, and health information storage and exchange, among others.
In the United States, healthcare providers are encouraged to use EMR/EHR systems. They are given financial benefits when they start using 'Meaningful EHR'. For the creation of information exchange facilities, the US government provides financial support to the community once they decide to build it.
To provide cost effective solutions to public healthcare facilities, countries have made use of open-source solutions. A large number of public healthcare facilities in the United States use the VISTA EHR system. It is available in the opensource domain. In England, the NHS encourages the use of open-source software solutions, and such solutions are operational in several places.
In some countries, personally controlled health records (PCHRs) or personal health records (PHRs) have been used for the exchange of health information when a patient moves from one provider to another. An example is Australia, where a PHCR system is used for the exchange of health information among the healthcare providers [19].
The second dimension is policy and regulations. Most countries have formulated national health IT policies that covers a spectrum of issues, such as the way health information is collected and shared. Different countries have formulated different policies to push the adoption of EHR systems. For example, in some countries, every healthcare provider has to create a summary record to be stored in a central place, whereas in other countries, the health information is distributed and is accessed when it is needed.
Regulations have been enacted for privacy protection, enabling the exchange of health information for the collection of patient information for use in clinical research and other purposes. In the United States, the Health Information Portability and Accountability Act (HIPAA) has existed for a long time. The rules of the HIPAA are more stringent for electronic records. In some countries, the privacy issue has been dealt with under acts that have been enacted to protect the privacy of any kind of personally sensitive information. For example, in Korea, privacy issues are covered by various acts, including the Telecommunications Business Act, the Protection of Communications Secrets Act, etc.
In Canada, the Personal Information Protection and Electronic Documents Act (PIPEDA), which protects personal information against improper collection, use, and disclosure, was extended to the healthcare sector in 2002. These laws also deal with the rights of patients as well as the powers of the government regarding the collection of data for various purposes. In most cases, data can be used after annonymization only.
Standards & interoperability is the third area of activity. Though international standards exist, there are several aspects which have to be looked into by every country as the processes used and infrastructure available in healthcare facilities differ from country to country. Country-specific meta-data standards have to be formulated and enforced to make systems interoperable.
The openEHR consortium [20] has developed an open and detailed specification of EHR. It has been adopted by several countries. The European Committee for Standardization has adopted many constructs of openEHR in its standard CEN EN 13606 prescribed for European Countries [21]. Other standards that are used in health IT applications include Health Level Seven (HL7) for exchange of messages [22], Digital Imaging and Communications in Medicine (DICOM) for representation, storage, and transmission of medical images [23], and the Continuity of Care Record (CCR) & Continuity of Care Document (CCD) for organizing the most relevant information for the purpose of the continuity of care.
Apart from these standards, there are several medical codes that are extensively used in the representation and storage of health information. The important ones include the International Classification of Diseases (ICD) of the World Health Organization [24], Systematized Nomenclature of Medicine - Clinical Terms (SNOMED-CT) published by SNOMED International [25] and Logical Observation Identifiers, Names and Codes (LOINC), which is primarily used in medical laboratories [26].
Most countries have established organizations to maintain standards in health IT. The US government supports agencies such as the Certification Commission for Health Information Technology (CCHIT) [27] and the Health Information Technology Standards Panel (HITSP) [28] to define needed functionalities, standardization of data exchange and collaboration among stakeholders. In Canada, Infoway has created the Standards Collaborative, which coordinates the development and adoption of standards.
Different countries have implemented different mechanisms for the generation of unique identification numbers for patients, which is necessary for interoperability. In New Zealand, the patient identity number system, called the "National Health Index" has existed for a long time. Its electronic version has been used in the implementation of EHR systems. In England, the NHS number is being used as patient identification number.
Governments are supporting R&D and human resource development for health IT. R&D is focused on the development of techniques to improve the quality of healthcare. Apart from the improved delivery of healthcare services, EHR is being used to improve clinical decision-making and to support decision-making for public health. In the United States, several projects have been funded under the Strategic HIT Advanced Research Projects (SHARP) Programme.
Schemes have been initiated to impart education and training in the area of health IT so that skilled manpower can be made available. The education and training programmes have been initiated for a range of medical and paramedical professions. Online courseware has been developed for training and retraining of the manpower.
The analysis of the strategies shows that there are several activities that have contributed significantly to the successful implementation of EHR systems. Some steps are countryspecific to deal with country-specific issues.
Figure 1 shows various components in the adoption of EHR. There are four broad components: ICT infrastructure, Policy & regulations, Standards & interoperability, and Research, development and education. The activities under each of these categories are listed in Table 1.
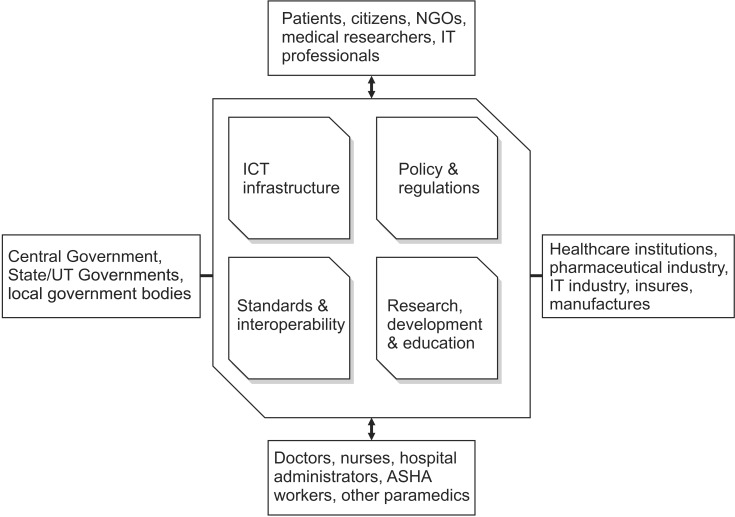
Components in Electronic Health Record (EHR) adoption.
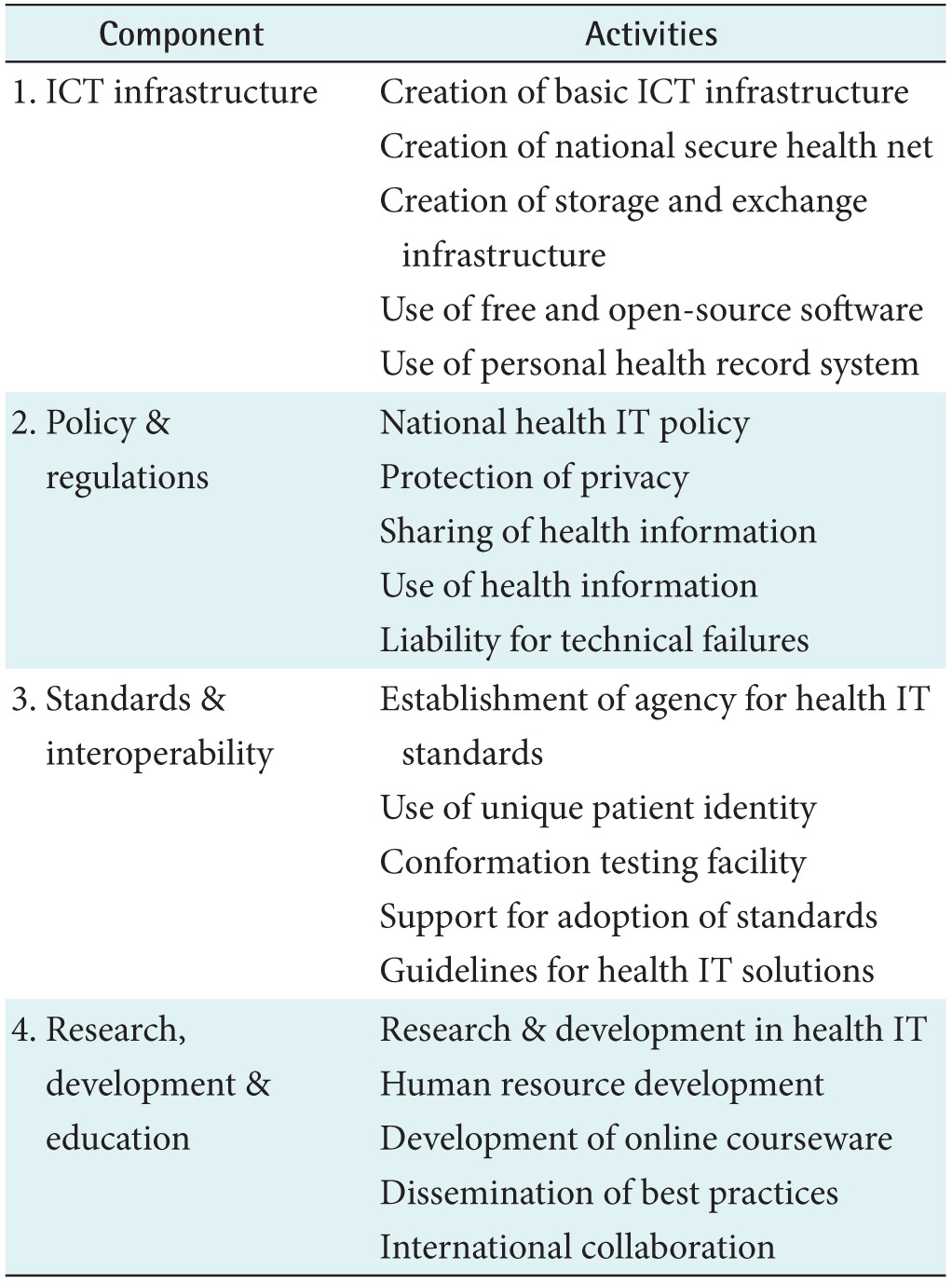
Activities in Electronic Health Record (EHR) adoption
4. Roadmap for India
In this section, we discuss how the crucial activities identified above can be carried out in the context of India. This provides a roadmap for the adoption of EHR in India. The roadmap identifies different tasks/activities that need to be taken up by various stakeholders to adopt EHR at the national level.
1) ICT infrastructure
(1) Basic ICT infrastructure
Public hospitals and dispensaries have very little ICT infrastructure. Only some major public hospitals, such as the All India Institute of Medical Sciences (AIIMS) and the Postgraduate Institute of Medical Education and Research (PGIMER), have computers and connectivity. The number of public healthcare facilities is quite large in the country; therefore, a large investment in hardware and software is required. To reduce expenses, it is necessary to use opensource software systems, mobile devices, and the cloud computing environment. With the implementation of the National Optical Fiber Network (NOFN), broadband connectivity will be available in every village. Once connectivity becomes available, cloud-based healthcare delivery can be brought to the village level.
(2) National secure health net
To exchange health information in a secure, reliable way, several countries have created communication networks connecting healthcare institutions. Such a network can be created on top of the existing National Knowledge Network (NKN), NICNET, ERNET, etc. Adequate privacy and security mechanisms have to be implemented to ensure the privacy and security of health information.
(3) Health information storage and exchange infrastructure
It is required for exchange of EHR among healthcare providers. A HIE finds patient data at other institutions using a master patient index, collects the information for the patient, and records the transaction for subsequent audit. HIE is also responsible for authentication of the person accessing the information while meeting the privacy requirements of the patient. The government needs to establish and maintain these exchanges in partnership with the private sector.
(4) Free and open-source EMR
As more than 75% of outpatients and more than 60% of inpatients are being treated in private healthcare facilities, it is necessary for the government to bring them on-board for using EHR. In view of the size of the country, there is a need to take an FOSS approach to making good quality software available to hospitals and individual practitioners. It should support all major national language scripts. If it is in the FOSS domain, even local entrepreneurs can provide technical support.
(5) Personal health record system
PHR or PCHR can play a significant role in adoption of EHR. PHR supports the adoption of EHR as the doctor does not have to start creating the record from scratch. The basic information, such as demographics, immunization details, known allergies, medical history, medical history of the family, test reports, etc. can be directly received from the PHR. On the other hand, once PHRs are available, patients can approach hospitals they have never visited before without worrying much about the interoperability issue.
2) Policy & regulations
(1) National health IT policy
The Central Government, in consultation with State Governments and other stakeholders, needs to formulate and announce a national health IT policy. Several efforts are already being made by the Central Government and State Government towards the use of IT in the healthcare delivery. The policy will ensure that the efforts being made lead to interoperable systems without duplication of effort.
(2) Protection of privacy
Regulations are needed to build trust in patients and providers while using e-health applications. Patients need to be assured that the confidentiality of their health data will not be compromised. Healthcare providers also have to be assured that whatever they record will not be altered without their knowledge. As the number of persons involved in the treatment process is quite large, it is necessary to have a rolebased access system.
(3) Sharing of health information
The benefits of EHR technology can be realized only when healthcare providers are able to share health information. At present, this does not exist except for the information given in relation to prescriptions and discharge summaries. The details of treatment and diagnosis are not available. Often healthcare providers are not willing to share information for several reasons. Laws are required to ensure that healthcare providers share information electronically in the interest of patients.
(4) Use of health information
The government needs to collect the health information of individual patients for use in public health decision-making or in clinical research. Legislation must provide a mechanism to use clinical information after necessary annonymization. Clinical decision-making may be subjected to medical audit for several purposes; therefore, the records must be made available for a reasonable period.
(5) Liability for technical failures
Another area which needs to be addressed by a regulatory framework is liability in case of technical failure, arising from malfunction of the system, communication channel, or unavailability of service, which can cause harm to the patient. Due to uncertainty, new players find it quite difficult to deal with it. Though it is necessary to hold people responsible for their failures to provide timely quality service, the regulations should specify the responsibilities of stakeholders so that they are aware of their responsibilities and do not suffer for reasons beyond their control.
3) Standards & interoperability
(1) Agency for health IT standards
Though standards have been prescribed by Ministry of Health & Family Welfare for various purposes, several steps need to be taken to facilitate adoption in the country. This is a continuous process; therefore, an agency should be given the responsibility to update continuously through an ongoing dialogue. The agency has to provide necessary technical support to other organizations in its implementation.
(2) Use of unique patient identity
At present, each hospital has its own way of giving a patient number to each visiting patient, but these are not recognized outside the organization. A consensus is needed on how to assign a number to each patient. The Aadhaar number given by the Unique Identity Authority of India (UIDAI) appears to be a good solution. As the seeding of the Aadhaar number is not 100%, an alternate mechanism has to be put in place. An algorithm has to be prescribed for use when the Aadhaar number is not available.
(3) Conformance testing facility
Even when standards are prescribed, often products and solutions developed need to be tested by an agency to verify that the solutions are interoperable. For example, several IT solutions, which claim to conform to HL7, do not interoperate with each other when they implement optional features of HL7 in different ways. The government should put a mechanism in place to empanel agencies for this purpose.
(4) Support for standards adoption
Support is needed in several forms. Facilities for training need to be created so that an adequate number of professionals can be trained. There are several legacy health IT systems which are operational in public healthcare facilities. These healthcare facilities should be supported for transition to standards compliant systems.
(5) Guidelines for health IT solutions
There are many areas where it may not be possible to mandate standards as it may be a hindrance for innovation. In such cases, there is often the possibility of issuing guidelines for the benefit of stakeholders.
4) Research, development & education
(1) Research & development in health IT
There is a need to support R&D projects on secondary usage of EHRs to support decision-making in public health, new methods of protection of privacy, etc. These projects can reduce the cost of deployment and improve the quality of service.
(2) Human resource development in health IT
A large number of IT professionals with exposure to health IT will be required to staff the IT unit of healthcare organizations. At present, no Indian university offers any master- or doctoral-level degree in this area. Steps need to be taken to start such courses in some of the institutions in the country.
(3) Development of online courseware
There is a need to start a programme to develop learning modules that can be used by anyone in the country. Training or retraining of a large number of professionals is expensive and time-consuming. The use of online courses solves the problem to some extent. An agency may be entrusted to issue certificates to eligible persons.
(4) Dissemination of best practices
In any emerging area, it is important to share experience periodically. An agency needs to collect such information and make it available at a central place. Though online sharing has to continue on a regular basis, workshops/conferences play their own role where people can discuss matters face to face.
(5) International collaboration
As India is lagging behind other nations in this area, it can benefit from international cooperation through access to their experience and IT solutions.
IV. Discussion
From the above, it is clear that implementation would be possible only with the joint efforts of all the stakeholders which include the Central Government, State Governments, healthcare providers, medical associations, IT industry, etc. Though an integrated initiative has not been started in the country, several works have been initiated which are leading to the implementation of EHR. Some of these are mentioned below briefly.
A system called e-hospital has been developed for use in hospitals and dispensaries across the country [29]. At present, it is running in about 50 hospitals. AIIMS, New Delhi [30] has implemented an IT solution to automate various processes and is working to develop other modules. The solution is being replicated in other institutions.
The Ministry of Health & Family Welfare has taken several steps to create standards. It has issued guidelines for EHR standards and meta-standards. It is also in the process of creating the National e-Health Authority (NeHA), which will look after standards related matters [31]. It is also revising other regulations to deal with the issue.
The Ministry is implementing an IT system for the processing of insurance claims under the new National Health Protection Scheme. The Ministry is also implementing the National Medical College Network project to provide connectivity for telemedicine. Another initiative in the area of use of IT in the healthcare sector is the National Health Portal [32].
The Ministry of Electronics & IT has been supporting the development and deployment of digital health solution for a long time. It has deployed telemedicine systems in several states in the country. It has sponsored R&D projects in various areas, including EMR system for oncology (at Regional Cancer Centre, Thiruvavanthapuram), PHR management system, technology for HIE, among others. In the past, it also created two working groups that prepared the reports "Recommended Guidelines and Standards for Practice of Telemedicine in India" [33] and "Framework for Information Technology Infrastructure for Health in India" [34]. These documents were extensively used in the finalization of standards in health IT. It created a resource centre the Centre for Development of Advanced Computing (C-DAC) Pune for standards in the area of health IT.
In conclusion, a number of countries have launched national initiatives to develop ICT-based health solutions including EHR systems and have progressed well despite several hurdles. Though an ideal situation in which every citizen has his/her EHR stored and it can be accessed throughout the country has not yet been achieved fully, substantial progress has been made. The adoption of EHR requires several technological and non-technological interventions, including standards, regulatory frameworks, etc. Different countries have taken different approaches as healthcare systems vary from country to country.
Though India has progressed well in the adoption of ICT in other sectors, such as banking, railway reservation, etc., and has an established IT industry, it has not yet utilized the potential of ICT in the healthcare sector. In public healthcare institutions, the usage of ICT is limited to billing and registration. The private sector has a limited form of EMR but it has not yet started the exchange of health information to improve quality of care. However, the situation is changing due to the efforts being made by the government and industry.
This report has presented a roadmap for the adoption of EHR systems to make use of the opportunity offered by ICT in the healthcare sector. This gives broad directions for moving ahead. Stakeholders need to make a coordinated effort to move forward.
Acknowledgments
The author would like to thank the government of India, Ministry of Electronics & Information Technology (MeitY) for providing the opportunity to prepare this report. The author had discussions on these issues with several IT experts and domain leaders at various forums. The author would like to thank each of them.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.