SMART Careplan System for Continuum of Care
Article information
Abstract
Objectives
This paper describes the integrated Careplan system, designed to manage and utilize the existing Electronic Medical Record (EMR) system; the system also defines key items for interdisciplinary communication and continuity of patient care.
Methods
We structured the Careplan system to provide effective interdisciplinary communication for healthcare services. The design of the Careplan system architecture proceeded in four steps-defining target datasets; construction of conceptual framework and architecture; screen layout and storyboard creation; screen user interface (UI) design and development, and pilot test and step-by-step deployment. This Careplan system architecture consists of two parts, a server-side and client-side area. On the server-side, it performs the roles of data retrieval and storage from target EMRs. Furthermore, it performs the role of sending push notifications to the client depending on the careplan series. Also, the Careplan system provides various convenient modules to easily enter an individual careplan.
Results
Currently, Severance Hospital operates the Careplan system and provides a stable service dealing with dynamic changes (e.g., domestic medical certification, the Joint Commission International guideline) of EMR.
Conclusions
The Careplan system should go hand in hand with key items for strengthening interdisciplinary communication and information sharing within the EMR environment. A well-designed Careplan system can enhance user satisfaction and completed performance.
I. Introduction
Patient safety and care are basic rights for patients in hospitals. Patient safety is defined as the avoidance, prevention, and amelioration of adverse outcomes or injuries stemming from the process of care [1,2,3] and any failure of system and human aspects across the patient care may cause adverse event occurrence. Adverse events related to medical care include all errors, mistakes, or accidents regardless of the existence of harm to patients [1,2], which lead to poor quality of care and greater cost. The Joint Commission, a US nonprofit organization for healthcare accreditation, emphasizes that teamwork is a critically important strategy for the prevention of adverse events and provision of a safe environment. In complex healthcare situations, teamwork promotes multidisciplinary cooperation and effective communication, which has a subsequent positive impact on safety culture and patient satisfaction [3,4]
Patient safety strategy related to information technology (IT) is effective in improving healthcare quality and reducing malpractice [5,6]; therefore, the implementation of health IT is recognized as an effective method to enhance healthcare quality and safety. If the architecture of health IT is poorly designed or has poor user interfaces and makes work flow more complicated, it can create hazards for patient safety and difficulties in clinical decision-making [2,6]. Thus, it is necessary to prepare a well-designed system, and furthermore, to prepare a well-integrated IT system within an Electronic Medical Record (EMR) environment, for accurate gathering of patient information with collaboration and communication between organizations [3,4,5,6].
The main reason for a healthcare organization's existence is patient care. To support and respond to each patient's unique needs and provide the most appropriate care requires a high level of planning and coordination [3].
Patient care uses data from various types of assessment, such as physical examination, health history, and an evaluation of physical, psychological, social, and economical factors across multiple care settings and departments and services. Healthcare practitioners identify and prioritize care and treatment to be provided to an individual patient using those data and revise the plan of care based on changes in the patient's condition as needed. A careplan is a record of the integrated care process, which involves prioritized problems, goals, target dates, and its revision history.
Considering dynamic and complicated healthcare settings, the development of a Careplan IT system can be a useful strategy to support effective communication and multidisciplinary cooperation and to improve patient safety in medical services.
In this paper, we describe Severance's integrated Careplan system, which was designed to manage and utilize the existing EMR. The system also defines key items for interdisciplinary communication.
II. Case Description
Designing the Careplan system architecture proceeded in four steps.
Step 1: Defining target datasets and making a conceptual framework
We established a conceptual framework based on reviewing the domestic medical certification and the Joint Commission International (JCI) guidelines. The conceptual framework includes target datasets and items from care delivery for all patients, care of high risk patients and provision of high risk services, food and nutrition therapy, pain management, and end-of-life care according to a care process.
Step 2: Construction of the main user interface (UI) and its architecture based on the conceptual framework
We used Microsoft Visual Studio .NET with C# 2012 (Microsoft, Redmond, WA, USA) and the DBMS was Microsoft SQL Server 2008. To determine the arrangement and construction of each UI and related datasets in the Careplan system, we operated a Careplan task force team (TFT) for six months.
Step 3: Screen layout and storyboard making
The basic strategy, 'using regardless of type of health care practitioner' was conceptualized. Therefore, the Careplan system was designed for integration and specialization at once. We were able to create a summary screen and detailed sub screens to be used for each need.
Step 4: UI design and development, and implementation
We completed the scope of UIs and functions through review by the Careplan TFT and quality improvement (QI) experts in addition to step-by-step evaluation by an International Patient Safety Group (IPSG) TFT.
An overview of the Careplan system and its architecture is shown in Figure 1.

Overview of the Careplan system and its architecture. EMR: Electronic Medical Record.
The conceptual framework includes sections and elements from care delivery for all patients as show in Table 1.
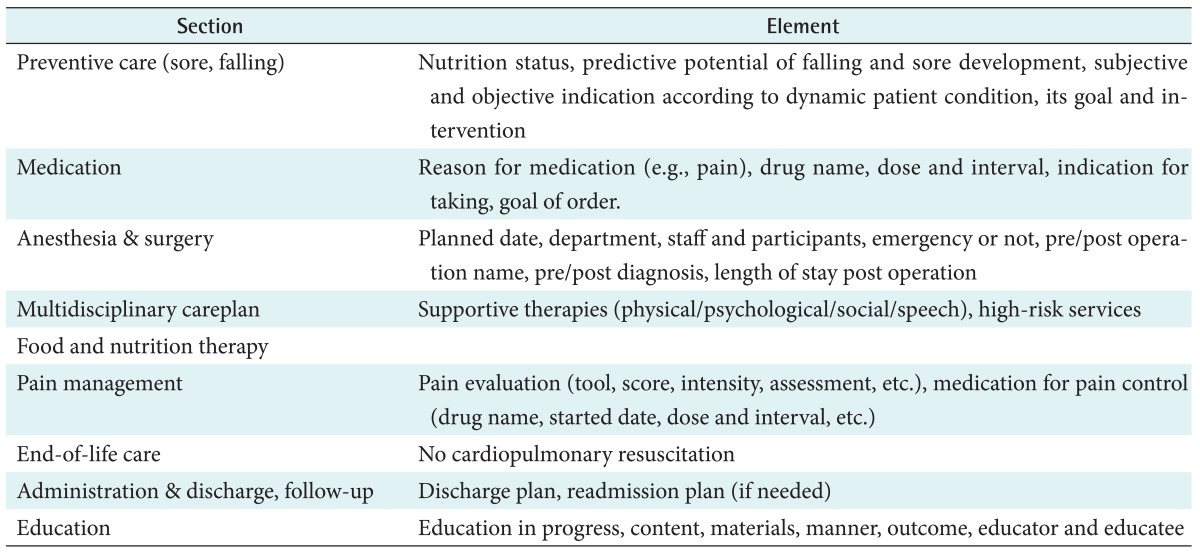
Section and elements for developing of the Careplan system
The Careplan system has client UIs and algorithms to retrieve each dataset. When a user selects a patient, the Careplan system will spontaneously display information that leaders and healthcare practitioners should know for preventive, palliative, and rehabilitative care. Information can reflect newly created datasets to receive medical records and information from the EMR system matched with the algorithms. The Careplan system reviews and writes a newer careplan and its goals directly. Figure 2 shows the main screen of the Careplan system rendered from the process described above.

Main screen of the Careplan system.
Each section represents characterized information served as data sources from the EMR system server. A data recorder with the pre-defined role of recomposing data to structured datasets. Additionally, if a user wants to know more detailed information and data sources, the Careplan system can provide related clinical documents or specific records from the hospital information system (HIS) according to the rule of the category master (Figure 3).
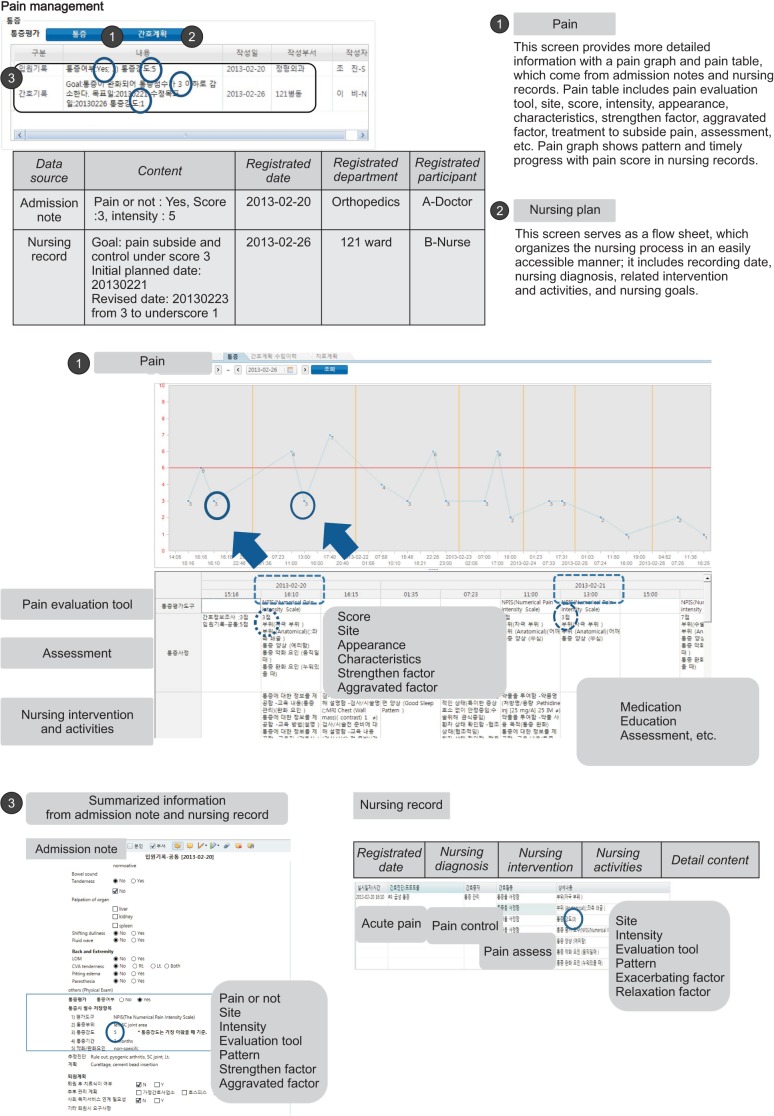
Division of pain management including its structure and details.
III. Discussion
The Careplan system could be expanded to include all healthcare participants who are involved in a patient's care step-by-step.
To begin applying the Careplan system within a hospital, it is difficult to understand what the Careplan is and why there is a need to establish a Careplan despite the fact that the EMR system with diverse handover is already being used. In our study, there was not enough awareness to share among health participants. The Careplan system is not only be a system for organizing care; rather, it also defines conceptual activities itself and creates a bridge between scattered data and guidelines to provide proper service with a uniform level. As time passes, most health participants may realize how important an overall careplan is in providing efficient, high-quality healthcare. However, the performance was not improved as much as we expected. One possible reason is that the participants did not have enough time, and they may have felt some difficulty in making careplans and measurable goals.
The Careplan system focuses on how establishing a careplan that should be systematized, of a high quality level, and individualized. Integrated client UIs and algorithms can reduce work burdens and provide accessibility to each data source (e.g., EMR documents and many types of order).
We discovered key elements for strengthening interdisciplinary communication and information sharing and developed the Careplan system for users to create careplans within an EMR environment. After expanding the Careplan system, we evaluated it by means of a survey, and we analyzed the factors influencing user satisfaction and performance to complete careplans. The most interesting result is that health participants (e.g. therapists) in a supported department show the highest user satisfaction. Additionally, employees who had been working 7-9 years had the highest recognition of careplans by working years, and employees who had been working for less than 1 year showed high user satisfaction.
Careplan recognition, system quality, and information quality led to varying results of user satisfaction [7,8]. Also, our analysis showed that the enhancement of system quality and information quality and continuous training support from organizations are factors that improve user satisfaction considering organization factors, such as how much top management buy-in had a positive effect on user satisfaction [8].
The results show that the Careplan system can play an important role in assisting leaders and health participants in the real planning and completion of careplans, visualization of careplans, convenience, sharing of careplans between departments, and training regarding careplan concepts and usage.
Acknowledgments
This study was supported by a grant from the Korea Health R&D Project, Ministry of Health & Welfare, Republic of Korea (No. HI13C1485).
Notes
No potential conflict of interest relevant to this article was reported.