Simulation Education Incorporating Academic Electronic Medical Records for Undergraduate Nursing Students: A Pilot Study
Article information

Abstract
Objectives
Academic electronic medical records (AEMRs) can be utilized for a variety of educational programs that can enhance nursing students’ nursing informatics and clinical reasoning competencies. This study aimed to identify the applicability and effectiveness of Simulation Education Incorporating AEMRs.
Methods
We developed simulation education scenarios incorporating AEMRs and evaluated them with 76 third- and fourth-year nursing students from five nursing schools using a mixed-methods design. We incorporated three simulation case scenarios involving preeclampsia, diabetes mellitus, and myocardial infarction into the AEMRs. After the simulation education, participants’ feedback on the usability of the AEMR system and their self-efficacy for AEMR utilization were collected via self-reported surveys. Subsequently, the simulation education incorporating AEMRs was evaluated through a focus group interview. The survey data were examined using descriptive statistics, and thematic analysis was done for the focus group interview data.
Results
The average mean scores for the AEMR system’s usability and participants’ self-efficacy for AEMR utilization were 5.36 of 7 and 3.96 of 5, respectively. According to the focus group interviews, the participants were satisfied with the Simulation Education Incorporating AEMRs and recognized their confidence in AEMR utilization. In addition, participants addressed challenges to Simulation Education Incorporating AEMRs, including the need for pre-education and AEMR utilization difficulties.
Conclusions
Nursing students were satisfied with and recognized the value of Simulation Education Incorporating AEMRs. Although the actual application of simulation education incorporating AEMRs remains challenging, further research can help develop and implement this approach for nursing students.
I. Introduction
Electronic medical records (EMRs) are essential elements of clinical information systems that share patient information in clinical settings [1]. In early 2000s, the Institute of Medicine of the United States emphasized that informatics abilities, including EMR utilization skills, were essential for health professionals [2]. Similarly, in 2021, the American Association of Colleges of Nursing proposed that nursing informatics competencies be included in nursing curricula for students to learn how to use EMRs [3]. To provide safe and effective nursing care, nurses are expected to utilize healthcare informatics and technologies, and new nursing graduates, nursing students, and nurse educators acknowledge the importance of EMR training [3,4]. A study reported that repeated EMR education and exposure enabled nursing students to feel confident using EMRs [5]. The educational exposure to informatics supported by academic electronic medical records (AEMRs) increased nursing students’ clinical practicum experience and clinical nursing awareness [6]. Despite the increasing demand for EMR instruction in nursing education, EMR-based educational programs remain limited [7,8]. In the classroom and during the clinical practicum, nursing students have limited opportunities to use EMRs [9], which reduces their self-efficacy for EMR utilization and makes it difficult for them to acquire EMR skills even after they become nurses [10,11].
Compared to conventional simulation education, simulation education incorporating AEMRs provides more training opportunities for nursing students to understand patients’ data in a structured context and judge their condition from the AEMR. For instance, in conventional simulation education, or problem-based learning, mainly paper-based medical records are provided to nursing students [12]. Providing patient data on paper differs from the reality and complexity of EMR in a clinical setting. Simulation education incorporating AEMRs can provide training opportunities for nursing students to choose essential data for the nursing process from the complex EMR environment and improve their integrated clinical reasoning competencies [13].
Therefore, this study aimed to identify the applicability and effectiveness of a pilot simulation education program incorporating AEMRs for future nursing education development strategies. In simulation education, one of the most important factors is the fidelity of the environment in which the simulation is conducted [14]. In this study, AEMRs were used to increase the clinical realism of the simulation environment.
II. Methods
1. Study Design
This study employed a mixed-methods design, with a one-group posttest only design and focus group interviews.
2. Participants and Settings
Third- and fourth-year nursing students at five nursing schools in South Korea participated in this study. Participants engaged in simulation education incorporating AEMRs for 2 hours, including a prebriefing, simulation, and recording of the nursing process and activities, at their nursing school’s simulation center. To ensure that participants felt comfortable, our research team conducted the study at their affiliated institutions. This study was conducted while avoiding regular subject hours or clinical practicum periods to encourage voluntary participation in research without credits or grades being affected. No participants withdrew during the study, and all participants completed their surveys without any missing records.
3. Scenario Development and AEMR Preparation
Our research team developed three case scenarios for the simulation: (1) a pregnant woman with preeclampsia, (2) an older patient with diabetes mellitus, and (3) a postoperative myocardial infarction. The purpose of developing three scenarios with comparable levels of difficulty was to prevent participants from sharing information. These scenarios required students to acquire the necessary information via the AEMR and solve the patients’ problems during simulation education. For instance, a student assigned to the postoperative myocardial infarction scenario was expected to assess the patient’s physical status while also reviewing the patient’s pre/postoperative coagulation battery, radiologic examination, electrocardiogram, and activity records to resolve the patient’s chest pain and dyspnea. The case scenarios for the simulation education were developed by adapting patients’ EMR data and case reports.
After the initial development of the scenarios, our team requested a validity review of each scenario from four nursing experts, including nurses and nursing professors with more than 3 years of clinical experience. Based on their feedback, the scenarios were modified. For instance, one professor suggested simplifying physicians’ prescription orders for educational purposes as nursing students may be confused by complicated prescriptions, even though the use of realistic prescriptions can be beneficial. Moreover, the simulation environments and supplies were suitable for simulation education incorporating AEMRs. We used high-fidelity manikins and standardized patients to suit the chosen case scenarios and nursing school environments.
For the AEMR application, we used Edge&Next, a cloud-based EMR application originally developed for hospital settings (ezCaretech, Seoul, Korea). Permission was obtained from ezCaretech, and the staff worked with the research team to modify the EMR application for our study. As this commercial, cloud-based EMR application was developed for use in hospitals, our research team modified the system for academic purposes while consulting the developers of the application. For example, we used a pre-set list of nursing diagnoses within the AEMR application. We added content lists for steps of the nursing process, such as assessment, planning, and evaluation, to allow nursing students to document nursing processes conveniently.
We pre-entered patient data, such as diagnosis, surgery history, allergies, physician’s prescription, symptoms, vital signs, medications, preventive nursing activities for falling and pressure ulcer prevention, laboratory data, radiologic examination data, nursing process documentation, and physical assessment data into the AEMR corresponding to the simulation case scenarios. Each student used an individual identification code to access and record the AEMR based on the assigned scenario.
4. Intervention
The intervention was conducted between December 2020 and February 2021. The simulation education incorporating the AEMR was conducted according to the protocol displayed in Figure 1. Each session of the simulation education program incorporating AEMRs consisted of three groups, with each group comprising two or three nursing students.
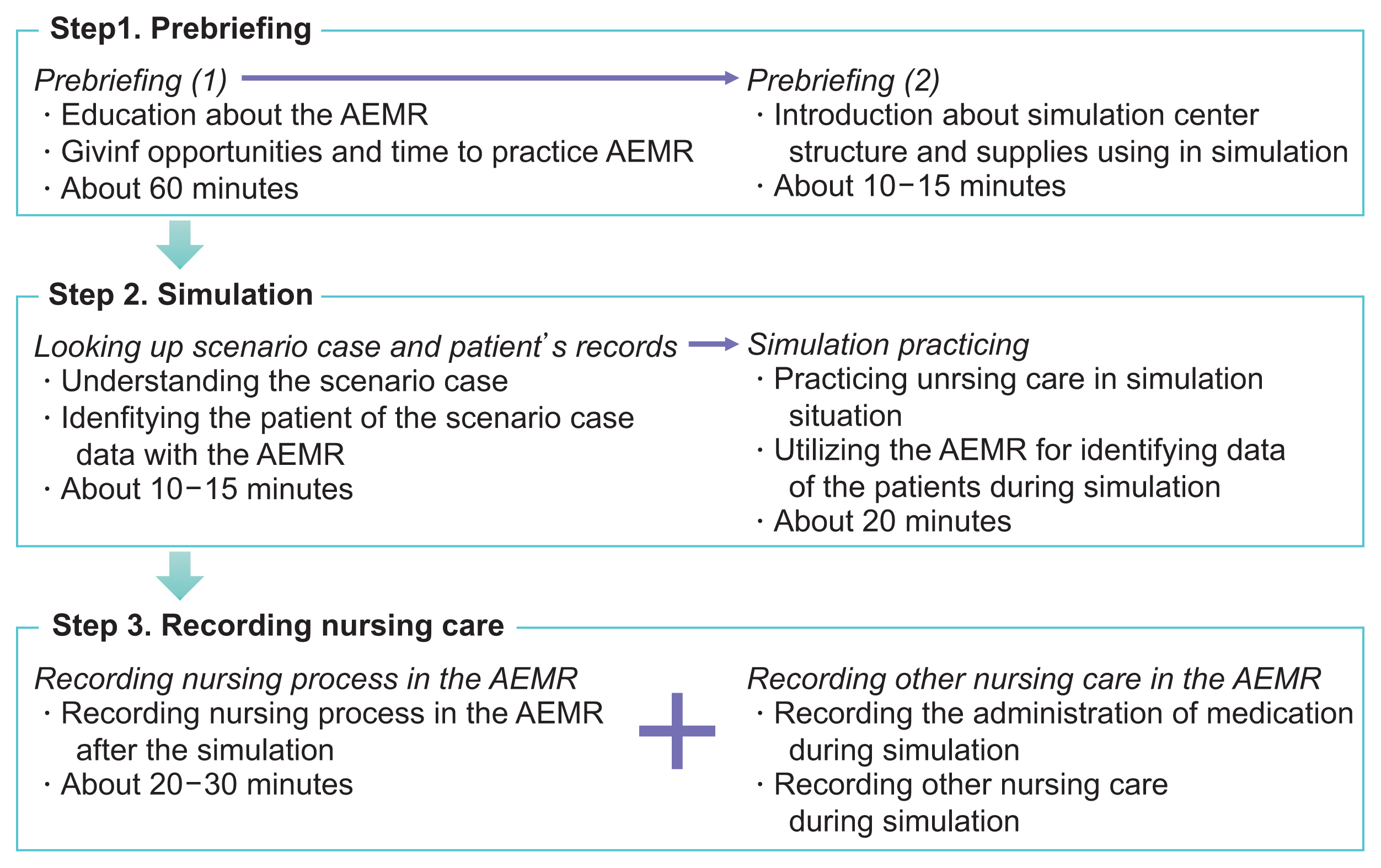
Protocol of operating the simulation education incorporating academic electronic medical records (AEMRs).
1) Step 1. Prebriefing
After obtaining informed consent, we performed a prebriefing that provided the simulation context, environment, supplies, and AEMR content to the participants. In this study, the prebriefing took place in two parts. The first stage was related to the use of the AMER. The AEMR categories and details were thoroughly described for participants to use during and after the simulation education incorporating AEMRs. Following that, participants were assured that sufficient time (approximately 60 minutes) and practice opportunities, would be provided throughout this process. During the second stage, participants became familiar with the simulation environment, including nursing supplies and operating procedures for 10–15 minutes.
2) Step 2. Simulation
The participants were provided a paper with the patient’s information and a scenario case outside the simulation room and had the opportunity to look up the patient’s records on the AEMR (Figure 2).
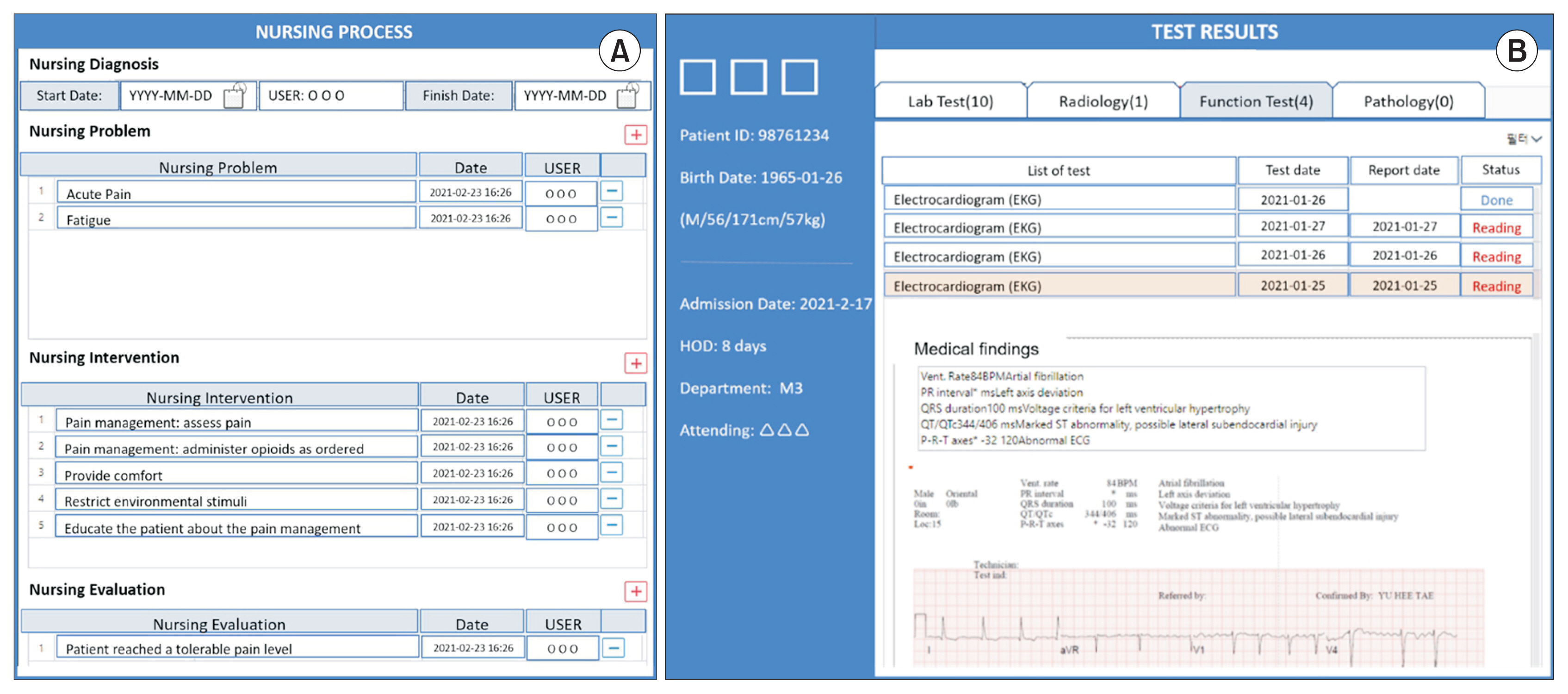
Content of the academic electronic medical record (AEMR) system included in this study. (A) An example of the nursing process. (B) An example of test results.
Participants entered the simulation room and performed physical examinations, therapeutic communication, nursing interventions, and interacted with other healthcare providers to solve problems. For instance, students were able to communicate with the physician via telephone, and the instructor who acted as the physician in the simulation prescribed the necessary medication. Participants also solved the nursing problem by utilizing updated data from the AEMR. The simulation lasted a total of 20 minutes.
3) Step 3. Recording on the AEMR
After completing the simulation, the participants recorded the clinical data and nursing process into the AEMR using individually provided laptops. Participants were requested to document two or more nursing processes and also record the nursing activities, such as medication administration, patient education, emotional support, and prevention of pressure ulcers.
5. Measurement
The self-reported survey items were general characteristics (gender, age, satisfaction with the nursing major, last semester’s grade point average, experience with AEMRs, and needs for AEMR-based nursing education), the usability of the AEMR system, and self-efficacy of AEMR utilization. As there were no appropriate tools to measure usability and self-efficacy for AEMR utilization, the research team modified or developed the scales. Five nursing professors—three experts in nursing informatics and two experts in nursing simulation education—evaluated the content validity of the scales used in this study.
The usability scale that was initially developed for mobile AEMR applications contained 22 items rated on a 7-point Likert scale that assessed perceived usefulness, ease of use, and user satisfaction [15]. The authors of the original scale gave approval for its use and modification. Cronbach’s alpha for each domain was 0.95.
The self-efficacy for AEMR utilization scale evaluated how confident nursing students were to utilize the AEMR after completing the program. The research team developed 10 items with a 5-point Likert scale, based on the mobile learning efficacy tool [16] and nursing students’ computer utilization responses and attitudes [17]. Cronbach’s alpha for self-efficacy for AEMR utilization was 0.94.
6. Data Collection
The participants responded to a self-reported survey after completing the simulation program. Among the participants, 26 voluntarily agreed to take part in focus group interviews in a semi-structured format. These focus groups included four to six participants per group (Table 1) and each focus group interview lasted between 60 and 90 minutes.

Semi-structured interview questions
7. Data Analysis
We used the descriptive statistics of frequencies, percentages, means, and standard deviations (SD) to analyze the participants’ general characteristics, the system’s usability, and the self-efficacy for AEMR utilization. The collected quantitative data were analyzed using SPSS version 26.0 (IBM Corp, Armonk, NY, USA). Thematic content analysis was conducted [18] for the interview content that was recorded and transcribed verbatim. We provided semantic codes corresponding to the relevant contents. After categories according to the relations among these codes were established, we were able to derive the key themes. Finally, we reviewed the relationships between each derived topic and the entire data set and generated accurate definitions through a cyclic process.
8. Ethical Considerations
To recruit participants, notices were posted on bulletin boards and a study presentation was held at five nursing schools. Researchers who had no connection with the students’ grades provided explanations and conducted the study. We did not provide additional benefits or grades as a reward for participation. All participants signed the written consent forms. After completing all procedures of simulation education incorporating AEMRs and evaluation, participants received a small gift as a token of appreciation. The Severance Hospital Institutional Review Board (No. Y-2020-0131) approved all study procedures.
III. Results
1. Demographic Characteristics
Most of the 76 participants were female (n = 68; 89.5%), in their fourth year (n = 59; 77.6%), satisfied with the nursing major (n = 63; 82.9%), and had a grade point average of 3.0 or higher (n = 71; 93.4%). Almost all students had no experience with AEMRs (n = 73; 96.1%), and agreed with the need for AEMR-based nursing education (98.7%) (Table 2).
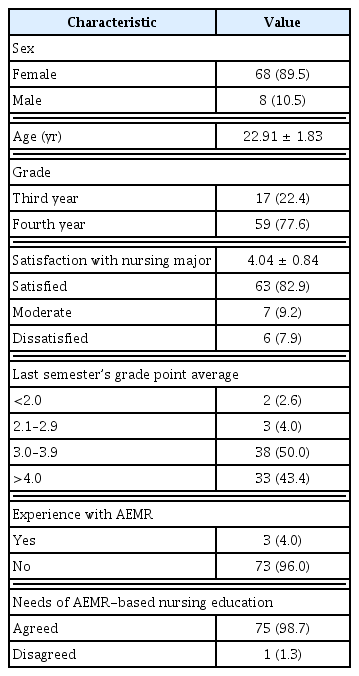
Demographic characteristics of participants (n = 76)
2. Usability, Self-Efficacy, and Nursing Process
The mean usability score was 119.28 ± 26.36 out of 154 (Table 3). The average mean value of “perceived usefulness” (5.61 ± 1.32) was lower than that of the other two domains: “user satisfaction” (5.56 ± 1.20) and “perceived ease of use” (4.89 ± 1.51). In perceived usefulness, “I would find the AEMR system useful in my practicum” (5.83 ± 1.53) had the highest score. All user satisfaction scores were higher than 5 out of 7. The scores of the items “intended to use the AEMR in the future” (6.00 ± 1.36) and “would recommend using the AEMR system for other students” (6.00 ± 1.54) were high.
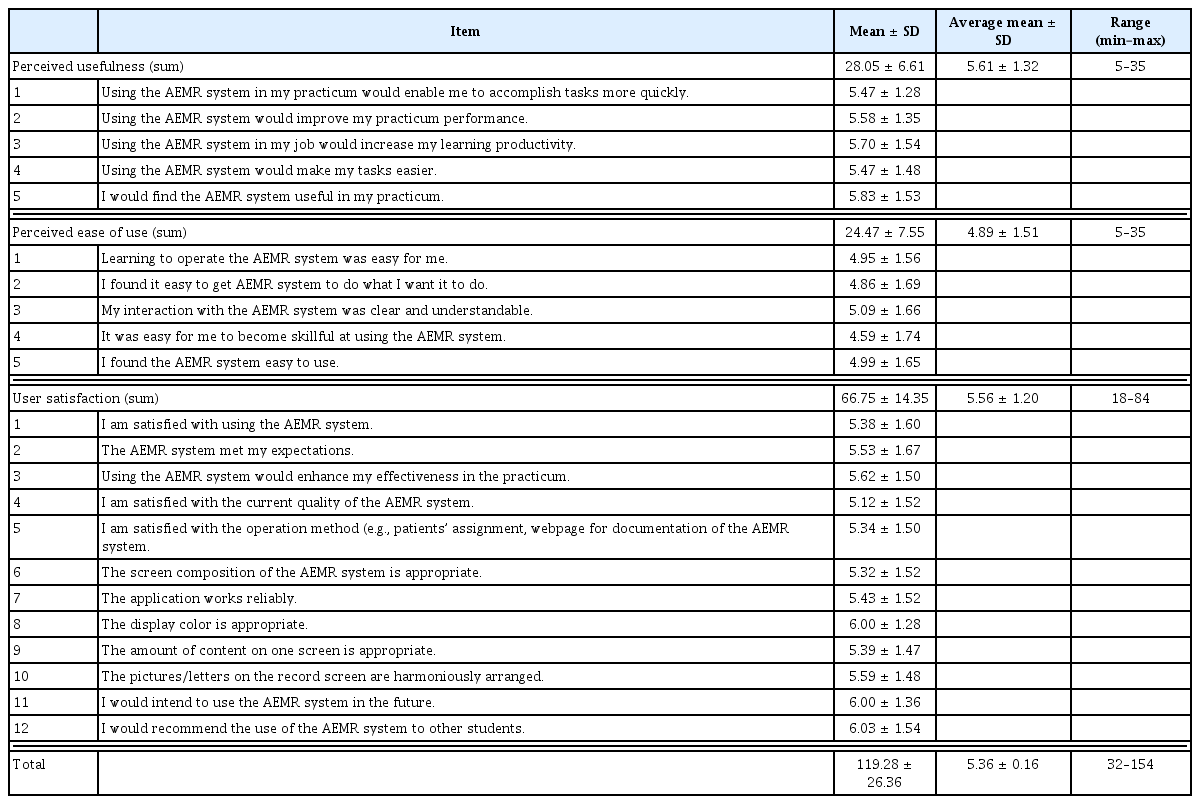
Usability of the AEMR system (n = 76)
The average self-efficacy for AEMR utilization after the simulation education was 39.63 ± 7.60 out of 50 (Table 4). Four items received average scores of over 4 out of 5. In particular, the participants expected the AEMR to be helpful in their learning (4.30 ± 0.85).

Self-efficacy of AEMR utilization (n = 76)
3. Focus Group Interview Findings
Tables 5 and 6 presented the focus group interview results. The participants discussed the benefits and challenges of the simulation education incorporating AEMRs. The themes related to benefits included immersion in simulation education, training for prioritization and information structuring, and confidence in actual EMR use (Table 5).

Benefits of the simulation education incorporating AEMR (n = 26)
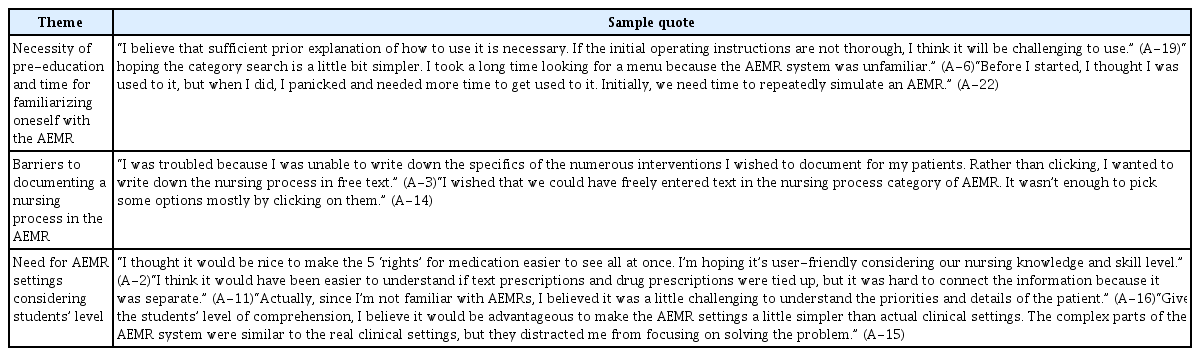
Challenges of the simulation education incorporating academic electronic medical records (n = 26)
The themes of challenges of the simulation education incorporating AEMRs were as follows: necessity of pre-education and time for familiarizing oneself with the AEMR, barriers to documenting a nursing process in the AEMR, and need for AEMR settings considering students’ level. Before becoming accustomed to the AEMR, the participants were uncomfortable and needed time to become immersed in the simulation education incorporating AEMRs. Participants stated that the simulation and AEMR educational content, including nursing process documentation and content difficulties, needed to be modified for nursing students (Table 6).
IV. Discussion
This study aimed to explore the applicability and effectiveness of simulation education incorporating AEMRs. Our research team expected that this simulation education incorporating AEMRs would enable nursing students to gain exposure to the problem-solving processes used by healthcare providers in clinical settings. Although the AEMR is not a novel concept, it is not widely used in nursing education in South Korea due to various factors, such as cost, personnel requirements, and time required for preparation and implementation. This study is meaningful as it recruited students from five nursing schools across the country to evaluate the advantages of using simulation education incorporating AEMRs with nursing students, as well as areas for improvement.
As the participants collected patient data through the AEMR system according to case scenarios, it was possible to obtain patient information, communicate with physicians and patients, and record the nursing process. This allowed students to experience realistic situations by immersing them in the simulation and to be an effective method of practice in a real-world setting as they expressed in focus group interviews. Increasing simulation education’s realism improves educational effectiveness [19,20]. Participants collected data that they considered necessary in the AEMR, allowing them to improve their clinical reasoning skills to analyze and synthesize patient data in a complex context [21,22].
Among the subgroups of AEMR usability, “perceived accessibility” had lower scores than “perceived usefulness” and “user satisfaction.” These findings corroborate those of a previous study in which the same measurements were used to evaluate mobile EMRs in clinical practicum [15]. Accordingly, participants stated that the AEMR increased educational effectiveness and satisfaction but was initially challenging to use. They found that using the AEMR was more complicated than they had anticipated, despite having the time and opportunity to practice prior to the simulation. Thus, simulation education incorporating AEMRs requires an adequate prebriefing or pre-education to acclimate students to the program. A prebriefing is critical for student engagement and self-confidence in simulation education [23,24]. We also discovered that when nursing students encountered difficulties with the overall simulation structure or environment, they focused on these issues rather than on the simulation education itself [24].
Following the completion of the program, we used a self-reported survey and focus group interviews to assess nursing students’ self-efficacy for AEMR utilization. Participants felt that simulation education incorporating AEMRs could benefit them and were confident in their ability to adapt. Related nursing informatics education is needed to provide nursing students with the knowledge and skills necessary to grasp the principles of AEMRs and usability methods (knowledge), and to practice becoming accustomed to the program (skill) with confidence (attitude) [25]. A case study in nursing pharmacology reported that AEMR improved students’ cognitive abilities to integrate AEMR data, medication data, and patient data [26]. Similarly, according to a previous scoping review, EMR training helped students develop positive attitudes toward and confidence in EMRs [27]. Healthcare providers need informatics education to assist them in resolving patient problems using clinical reasoning and health data. Undergraduate students require strategic approaches for the development of informatics competencies [3], as these cannot be acquired in a short time [28]. Thus, early and repeated practice and exposure can increase self-efficacy and, subsequently, enhance competencies of nursing informatics and clinical reasoning.
Participants stated some challenges to recording their nursing processes into the AEMR system. Although the AEMR system used in this study was modified to accommodate simulation education incorporating AEMRs, we identified that it was challenging for undergraduate students to record nursing processes. In particular, documenting nursing goals in the AEMR was not easy. During the focus group interviews, participants expressed their desire to record nursing processes in the AEMR with greater ease, for example, using free text in the AEMR. Thus, AEMRs should have the feature of recording nursing processes more conveniently, which is needed for educational purposes. Teaching nursing processes and effective recording methods have been emphasized recently in the literature. Similarly, as nursing records contain various free text fields [29], training for accurate and detailed EMR recordings is required.
1. Strengths and Limitations of the Study
The main strength of this study is that it provides evidence to promote simulation education incorporating AEMRs for undergraduate nursing students. It is pivotal to the expansion of simulation education utilizing EMRs to replicate real-world clinical situations [12]. Despite its strength, this study has some limitations. First, because it had a posttest-only, single-group design, our data support limited causal inferences. The interpretation should focus on the applicability and acceptability of simulation education incorporating AEMRs for third- and fourth-year nursing students who have participated in at least one semester of clinical practicum. Additionally, advanced educational programs utilizing AEMRs with various designs and larger sample sizes are also needed. For instance, interprofessional education can be conducted using AEMRs to foster interprofessional cooperation or communication skills.
2. Education and Research Implications
Based on the findings of this study, several implications for nursing education and research may be suggested. First, AEMRs should become an essential component of the curricula for nursing education, including health assessment, simulation, and clinical practicum through repeated use. This would help nursing students’ confidence and capacity to document the nursing process, use relevant information, and prioritize it for care planning. Second, the utilization of AEMRs will enhance the development of nursing students’ competencies in literacy and using health information to build clinical judgment and critical thinking. Third, to actively promote education and research that adopts AEMRs, developing a specific measurement that can evaluate the effectiveness of AEMR-related educational programs is crucial.
Acknowledgments
This work was supported by the Korean Society of Medical Informatics, and 2019 grant from the Yonsei University College of Nursing. Soomin Hong received a scholarship from the Brain Korea 21 FOUR Project funded by the National Research Foundation (NRF) of Korea, Yonsei University College of Nursing.
Notes
Conflict of Interest
Mona Choi is an editorial member of Healthcare Informatics Research; however, she did not involve in the peer reviewer selection, evaluation, and decision process of this article. Otherwise, no potential conflict of interest relevant to this article was reported.