
I. Introduction
Before the introduction of the Universal Coverage Scheme (UCS) in Thailand in 2001, approximately 30% of patients‚ÄĒparticularly children, the elderly, the unemployed, and workers in the informal sector‚ÄĒwere not covered by any of the then-existing health insurance and welfare schemes. Since the UCS was implemented, it has covered virtually the entire population. The scheme is administered by the National Health Security Office (NHSO) [1]. All public hospitals are mandated to join the UCS, while private hospitals may voluntarily participate. Under the UCS, reimbursement of hospitals for expenditures related to inpatient-care is determined by the diagnosis-related grouping (DRG) system, which provides retrospective payments within a global budget. Unfortunately, use of the DRG leads to coding adjustment and manipulation as hospitals attempt to report diagnosis and procedural codes that will allow them to receive larger reimbursements. In contrast, some data might be ignored simply because there is a lack of financial incentives for hospitals to report them. Some countries employ a ‚Äėreason for admission‚Äô rule as the basis for the principal diagnosis, while other countries employ a ‚Äėresource use‚Äô rule [2]. In Thailand, the reason for admission is used. A previous study found that nearly half (42%) of the principal diagnoses recorded in discharge summaries had been incorrectly reported [3]. Moreover, another study found that 48% of the sampled principal diagnoses had been miscoded [4].
The present study differed from previous studies in that it focused on the validity of the principal diagnoses recorded in summary and coding assessment forms, which classify disease systems and specific disease groups according to the International Statistical Classification of Diseases and Related Health Problems (ICD-10). The objective, methodology, design, and analysis (of medical records) of this study differed from those of previous studies, which examined coding practices and processes in hospitals [56]. This study compared data from discharge summaries with data obtained from medical-record reviews (as a gold standard), and in addition, compared data from coding assessments with data in the computerized ICD-10 (the database used for reimbursement purposes) and the discharge summaries (as a gold standard). All reference material was obtained from the ICD-10 [7], and ICD-10 Thai Modification (ICD-10-TM) Standard Coding Guidelines [8].
II. Methods
1. Study Population Group and Design
In this retrospective study, in 2015, secondary data from audit assessments were collected from the Bureau of Claims and Medical Audit, using the audit results from 2014. A total of 118,971 medical records were sampled. The Bureau of Claims and Medical Audit has set five criteria for its hospital audits: (1) reimbursements were more than 10 times the mean value (based on the overall value in Thailand); (2) results were corrected to less than the mean value in the preceding year; (3) the percentage of adjusted relative weight (RW) changes was more than the mean value; (4) the number of adjusted relative weight changes was more than the mean value; and (5) over-coding was more than the mean value. The samples comprised records from 505 government hospitals and 29 private hospitals participating in the UCS in Thailand.
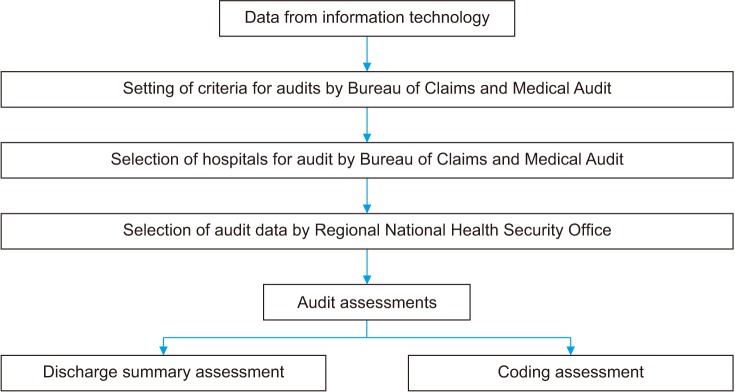
Audits were conducted of inpatient medical records showing abnormal data, such as those having procedures unrelated to the principal diagnosis, a very high patient clinical complexity level (PCCL = 4 ‚Äėcatastrophic‚Äô), a length of stay of less than 3 days, and an RW of more than 5. Three percent of the records were selected by systemic random sampling by the Regional National Health Security Office. The regional auditors, who had passed training assessments conducted by the Bureau of Claims and Medical Audit of the NHSO, comprised 762 doctors, 630 nurses, and 464 coders. The evaluation of each principal diagnosis consisted of a summary assessment and a coding assessment, both of which followed the guidelines contained in ICD-10 [7] and Standard Coding Guidelines in Thailand [8]. The principal diagnoses recorded in the summary assessments were audited by comparing the discharge summaries with data obtained from a review of the medical records. The principal diagnoses contained in the coding assessments were audited by comparing data in the computerized ICD (the database used for reimbursement purposes) and the discharge summaries (Figure 1). For each patient, the principal diagnosis recorded by a physician in the discharge summary must meet the following three requirements [8]: (1) only one principal diagnosis is to be recorded as the reason for admission; (2) if a patient has many major disease conditions, the disease that needs treatment and admission, the most severe disease, or the disease requiring the highest resource use must be selected; (3) if the physician cannot summarize the final diagnosis, or if there are unknown causes, then the signs and symptoms of the patient are to be used.
2. Analysis
The summary assessments of the principal diagnoses were audited by comparing the discharge summaries prepared by physicians with medical record reviews conducted by auditors (as the gold standard). The summary assessments were classified as being in agreement (i.e., having the same principal diagnoses), incorrect (i.e., there was a degree of difference between the discharge summaries and the medical record reviews), non-specific, or unjustified (i.e., there was no evidence in the medical records to support the principal diagnoses shown in the diagnostic summaries).
Using the concept of screening test validity from the field of epidemiology, the term ‚Äúsensitivity‚ÄĚ refers to the proportion of people with a disease in the screened population who were identified as ill by the screening test. The related term ‚Äúspecificity‚ÄĚ refers to the proportion of disease-free people who were so identified by the screening test. Similarly, the ‚Äúpositive predictive value‚ÄĚ refers to the probability of the disease being present in a patient with an abnormal test result, while the ‚Äúnegative predictive value‚ÄĚ is the probability of a patient not having a disease when a test result is negative [9]. For example, the sensitivity of the discharge summary assessments was calculated as the percentage of agreement with the relevant diagnoses contained in the discharge summaries and obtained from the medical records, using the medical record reviews undertaken by auditors as the gold standard (which are based on the criteria in the Standard Coding Guidelines, Thailand). The analysis measured sensitivity and specificity as well as positive and negative predictive values. Efficiency was assessed as the sum of the true positive and true negative values divided by the percentage of agreement.
The coding assessments of the principal diagnoses were audited by comparing the ICD and discharge summaries, by examining their level of agreement (i.e., having the same coding), by identifying the proportion that were incorrect (i.e., the difference between the computerized ICD and discharge-summary codings), and by ascertaining the proportion that had a non-specific diagnosis according to both the computerized ICD and discharge summaries. The analysis measured sensitivity and specificity as well as positive and negative predictive values using the discharge summary coding as the gold standard (SPSS Statistics ver. 18; SPSS Inc., Chicago, IL, USA).
III. Results
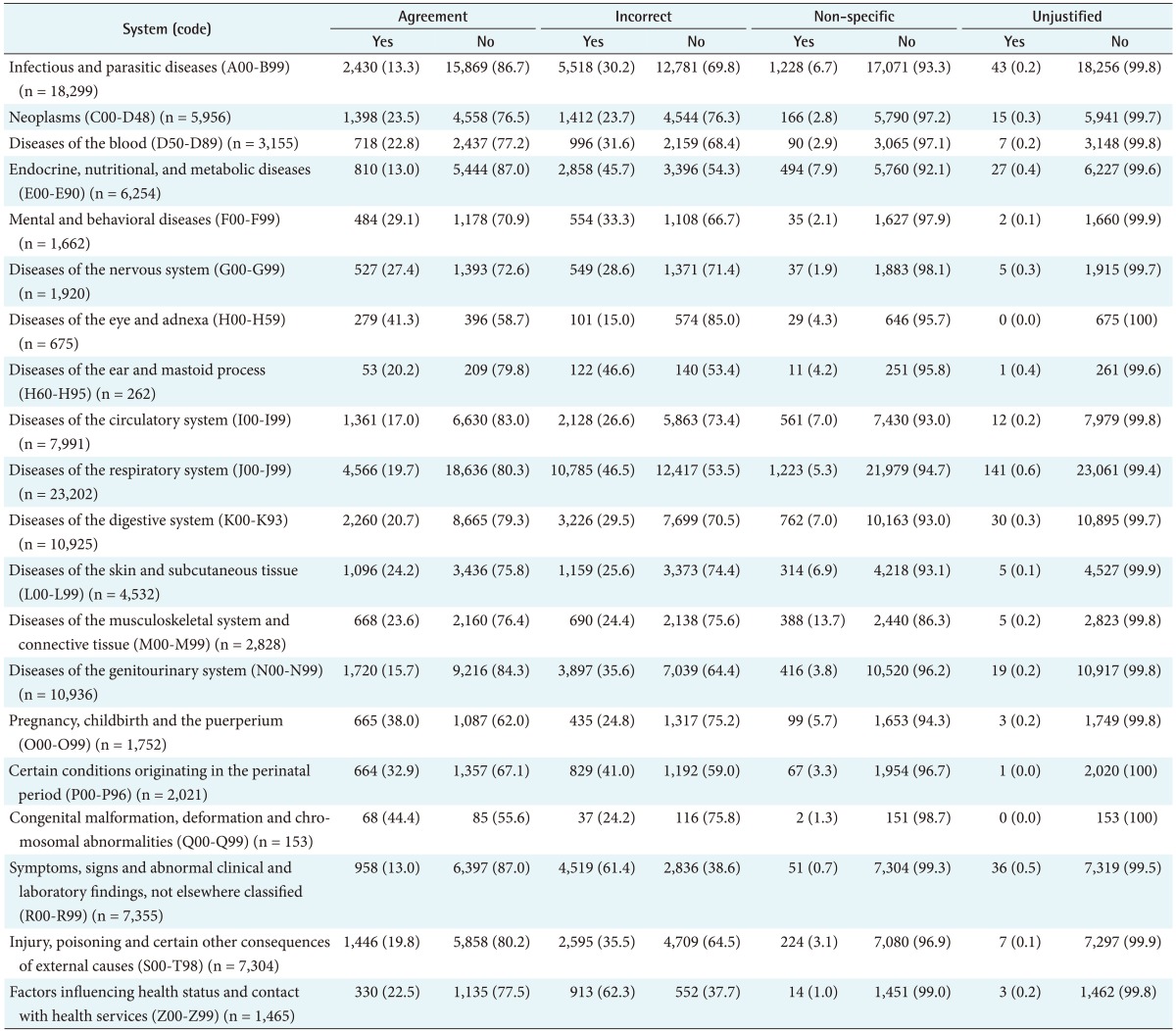
A comparison of the principal diagnoses given in the discharge summaries and the data in the medical record reviews (Table 1) showed the lowest level of agreement (87.0% disagreement) for the principal diagnoses for the categories ‚ÄúEndocrine, nutritional, and metabolic diseases‚ÄĚ and for ‚ÄúSymptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified‚ÄĚ. These were followed in decreasing order by the categories ‚ÄúInfectious and parasitic diseases‚ÄĚ (86.7% disagreement), ‚ÄúDiseases of the genitourinary system‚ÄĚ (84.3%), ‚ÄúDiseases of the circulatory system‚ÄĚ (83.0%), and ‚ÄúDiseases of the respiratory system‚ÄĚ (80.3%).
By contrast, the highest level of agreement for the principal diagnosis was for the category ‚ÄúCongenital malformation, deformation, and chromosomal abnormalities‚ÄĚ (44.4% agreement level), followed in decreasing order by ‚ÄúDiseases of the eye and adnexa‚ÄĚ (41.3%), ‚ÄúPregnancy, childbirth, and the puerperium‚ÄĚ (38.0%), ‚ÄúCertain conditions originating in the perinatal period‚ÄĚ (32.9%), ‚ÄúMental and behavioral diseases‚ÄĚ (29.1%), ‚ÄúDiseases of the nervous system‚ÄĚ (27.4%), ‚ÄúDiseases of the skin and subcutaneous tissue‚ÄĚ (24.2%), and ‚ÄúDiseases of the musculoskeletal system and connective tissue‚ÄĚ (23.6%).
The highest proportion of incorrect diagnoses was for the category ‚ÄúFactors influencing health status and contact with health services‚ÄĚ (62.3%), followed in decreasing order by ‚ÄúSymptoms, signs, and abnormal clinical and laboratory findings, not elsewhere classified‚ÄĚ (61.4%), ‚ÄúDiseases of the ear and mastoid process‚ÄĚ (46.6%), ‚ÄúDiseases of the respiratory system‚ÄĚ (46.5%), ‚ÄúEndocrine, nutritional, and metabolic diseases‚ÄĚ (45.7%), ‚ÄúCertain conditions originating in the perinatal period‚ÄĚ (41.0%), and ‚ÄúDiseases of the genitourinary system‚ÄĚ (35.6%).
Conversely, the lowest proportion of incorrect diagnoses was for the category ‚ÄúDiseases of the eye and adnexa‚ÄĚ (15.0% incorrect), followed in increasing order by the categories ‚ÄúNeoplasms‚ÄĚ (23.7%), ‚ÄúCongenital malformation, deformation, and chromosomal abnormalities‚ÄĚ (24.2%), ‚ÄúDiseases of the musculoskeletal system and connective tissue‚ÄĚ (24.4%), ‚ÄúPregnancy, childbirth, and the puerperium‚ÄĚ (24.8%), ‚ÄúDiseases of the skin and subcutaneous tissue‚ÄĚ (25.6%), ‚ÄúDiseases of the circulatory system‚ÄĚ (26.6%), ‚ÄúDiseases of the nervous system‚ÄĚ (28.6%), ‚ÄúDiseases of the digestive system‚ÄĚ (29.5%), and ‚ÄúInfectious and parasitic diseases‚ÄĚ (30.2%).
The highest level of agreement for a non-specified diagnosis was for the category ‚ÄúDiseases of the musculoskeletal system and connective tissue‚ÄĚ (13.7%), followed in decreasing order by the categories ‚ÄúDiseases of endocrine, nutritional, and metabolic diseases‚ÄĚ (7.9%), ‚ÄúDiseases of the circulatory system‚ÄĚ (7.0%), ‚ÄúDiseases of the digestive system‚ÄĚ (7.0%), ‚ÄúDiseases of the skin and subcutaneous tissue‚ÄĚ (6.9%), and ‚ÄúInfectious and parasitic diseases‚ÄĚ (6.7%).
The codings for the principal diagnoses were audited by comparing the computerized codes given in ICD-10 with those in the discharge summaries (Table 2). This study found that the lowest agreement for coding was for the category ‚ÄúInjury, poisoning, and certain other consequences of external causes‚ÄĚ (71.3%), followed in decreasing order by ‚ÄúPregnancy, childbirth, and the puerperium‚ÄĚ (64.4%), ‚ÄúCertain conditions originating in the perinatal period‚ÄĚ (61.9%), and ‚ÄúEndocrine, nutritional, and metabolic diseases‚ÄĚ (60.8%).
On the other hand, the highest agreement for coding was for the category ‚ÄúDiseases of the respiratory system‚ÄĚ (61.8%), followed in decreasing order by ‚ÄúMental and behavioral diseases‚ÄĚ (59.5%), ‚ÄúDiseases of the nervous system‚ÄĚ (56.7%), ‚ÄúInfectious and parasitic diseases‚ÄĚ, and ‚ÄúSymptoms, signs and abnormal clinical and laboratory finding, not elsewhere classified‚ÄĚ (55.5%).
The highest incorrect coding was for the category ‚ÄúFactors influencing health status and contact with health services‚ÄĚ (33.8%), followed in decreasing order by ‚ÄúPregnancy, childbirth and the puerperium‚ÄĚ (33.2%), ‚ÄúCertain conditions originating in the perinatal period‚ÄĚ (33.1%), and ‚ÄúEndocrine, nutritional, and metabolic diseases‚ÄĚ (30.6%).
The lowest incorrect coding was for ‚ÄúDiseases of the respiratory system‚ÄĚ (13.2%), followed in increasing order by ‚ÄúDiseases of the nervous system‚ÄĚ (14.1%), ‚ÄúDiseases of the genitourinary system‚ÄĚ (14.6%), and ‚ÄúDiseases of the digestive system‚ÄĚ (15.5%).
The highest non-specific coding was for ‚ÄúDiseases of the musculoskeletal system and connective tissue‚ÄĚ (6.8%), followed in decreasing order by ‚ÄúInfectious and parasitic diseases‚ÄĚ (1.9%), ‚ÄúDiseases of the circulatory system‚ÄĚ (1.9%), ‚ÄúDiseases of the skin and subcutaneous tissue‚ÄĚ (1.7%), and ‚ÄúCertain conditions originating in the perinatal period‚ÄĚ (1.7%).
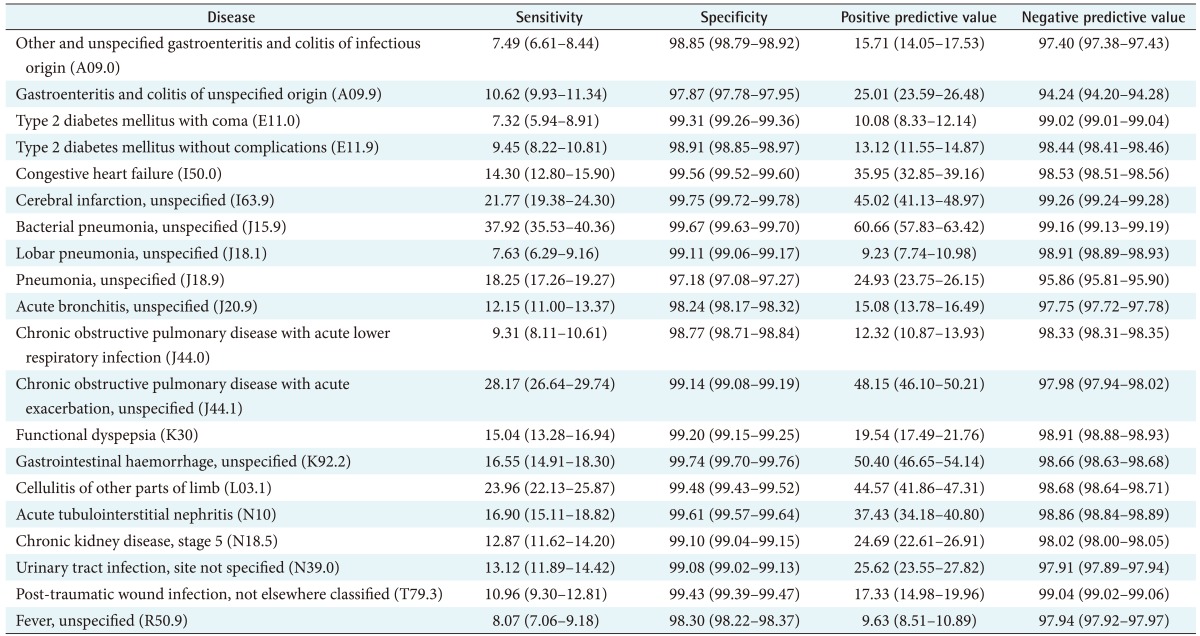
The validity of the principal diagnoses recorded in the discharge summaries was determined by comparing them with the medical-record review audits for the top-twenty principal diagnoses (Table 3). It was found that the category ‚ÄúBacterial pneumonia, unspecified‚ÄĚ had the highest sensitivity (37.92%), followed in decreasing order by the categories ‚ÄúChronic obstructive pulmonary disease with acute exacerbation, unspecified‚ÄĚ (28.17%), ‚ÄúCellulitis of other parts of limb‚ÄĚ (23.96%), and ‚ÄúCerebral infarction, unspecified‚ÄĚ (21.77%).
Conversely, ‚ÄúType 2 diabetes mellitus with coma‚ÄĚ had the lowest sensitivity (7.32%), followed in increasing order by ‚ÄúOther and unspecified gastroenteritis and colitis of infectious origin‚ÄĚ (7.49%), ‚ÄúLobar pneumonia, unspecified‚ÄĚ (7.63%), ‚ÄúFever, unspecified‚ÄĚ (8.07%), ‚ÄúChronic obstructive pulmonary disease with acute lower respiratory infection‚ÄĚ (9.31%), and ‚ÄúType 2 diabetes mellitus without complications‚ÄĚ (9.45%).
As for positive predictive values, the category ‚ÄúBacterial pneumonia, unspecified‚ÄĚ had the highest value (60.66%), followed by ‚ÄúGastrointestinal haemorrhage, unspecified‚ÄĚ (50.40%), ‚ÄúChronic obstructive pulmonary disease with acute exacerbation, unspecified‚ÄĚ (48.15%), ‚ÄúCerebral infarction unspecified‚ÄĚ, and ‚ÄúCellulitis of other parts of limb‚ÄĚ (44.57%).
In the case of the lowest positive predictive values, the category ‚ÄúLobar pneumonia, unspecified had the lowest value (9.23%), followed in increasing order by ‚ÄúFever unspecified‚ÄĚ (9.63%), ‚ÄúType 2 diabetes mellitus with coma‚ÄĚ (10.08%), ‚ÄúChronic obstructive pulmonary disease with acute lower respiratory infection‚ÄĚ (12.32%), and ‚ÄúType 2 diabetes mellitus without complications‚ÄĚ (13.1%).
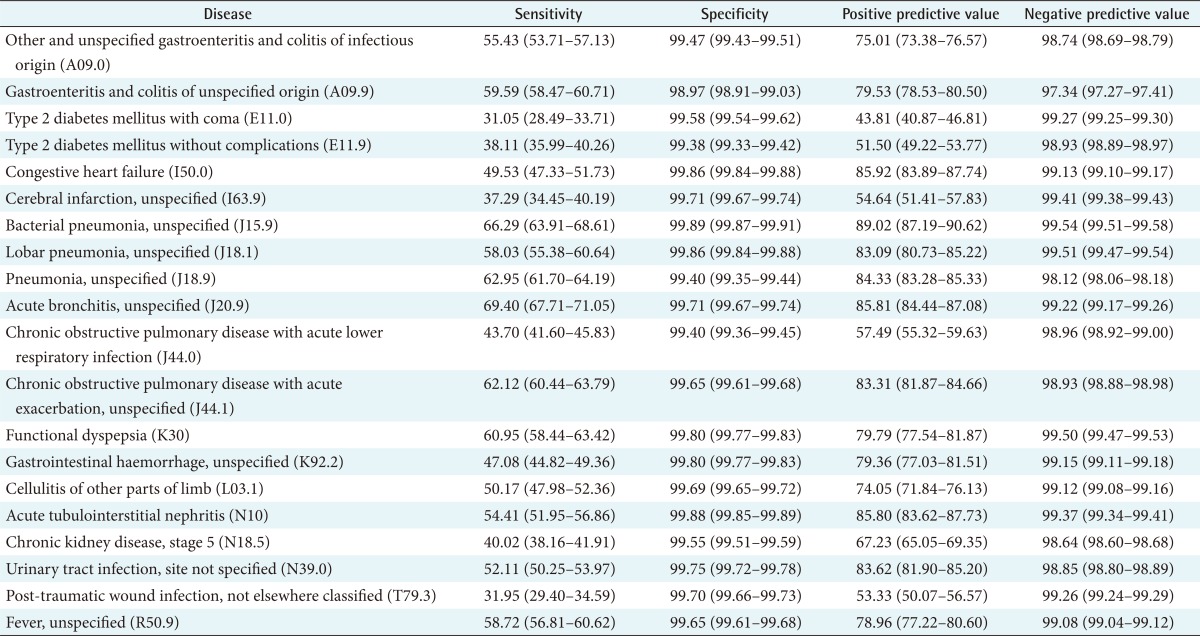
The validity of the codes used for the principal diagnoses recorded in the discharge summaries was determined by comparing them with the computerize ICD-10 codes for the top-twenty principal diagnoses (Table 4). It was revealed that the category ‚ÄúAcute bronchitis, unspecified‚ÄĚ had the highest sensitivity (69.40%), followed by ‚ÄúBacterial pneumonia, unspecified‚ÄĚ (66.29%), ‚ÄúPneumonia, unspecified‚ÄĚ (62.95%), ‚ÄúChronic obstructive pulmonary disease with acute exacerbation, unspecified‚ÄĚ (62.12%), ‚ÄúFunctional dyspepsia‚ÄĚ (60.95%), and ‚ÄúGastroenteritis and colitis of unspecified origin‚ÄĚ (59.59%).
In terms of the lowest sensitivities, ‚ÄúType 2 diabetes mellitus with coma‚ÄĚ had the lowest sensitivity (31.05%), followed in increasing order by ‚ÄúPost-traumatic wound infection not elsewhere classified‚ÄĚ (31.95%), ‚ÄúCerebral infarction, unspecified‚ÄĚ (37.29%), ‚ÄúType 2 diabetes mellitus without complications‚ÄĚ (38.11%), and ‚ÄúChronic kidney disease, stage 5‚ÄĚ (40.02%).
As for positive predictive values, ‚ÄúBacterial pneumonia, unspecified‚ÄĚ had the highest at 89.02%, followed in decreasing order by ‚ÄúCongestive heart failure‚ÄĚ (85.92%), ‚ÄúAcute bronchitis, unspecified‚ÄĚ (85.81%), ‚ÄúAcute tubulointerstitial nephritis‚ÄĚ (85.80%), ‚ÄúPneumonia, unspecified‚ÄĚ (84.33%), and ‚ÄúUrinary tract infection, site not specified‚ÄĚ (83.6%).
On the other hand, ‚ÄúType 2 diabetes mellitus with coma‚ÄĚ had the lowest positive predictive value (43.81%), followed by ‚ÄúType 2 diabetes mellitus without complications‚ÄĚ (51.50%), ‚ÄúPost-traumatic wound infection not elsewhere classified‚ÄĚ (53.33%), ‚ÄúCerebral infarction, unspecified‚ÄĚ (54.64%), and ‚ÄúChronic obstructive pulmonary disease with acute lower respiratory infection‚ÄĚ (57.49%).
IV. Discussion
Comparison of the principal diagnoses recorded in the discharge summaries with the details in the medical records revealed that the lowest level of agreement for the principal diagnoses was jointly shared by two categories: ‚ÄúEndocrine, nutritional, and metabolic diseases‚ÄĚ and ‚ÄúSymptoms, signs, and abnormal clinical and laboratory finding not elsewhere classified‚ÄĚ. In addition, the category with the highest proportion of incorrect diagnoses was ‚ÄúFactors influencing health status and contact with health services‚ÄĚ.
As for the coding of the principal diagnoses, it was audited by comparing the codes shown on the discharge summaries with the computerized ICD-10 codes. It was found that the lowest agreement for coding was for ‚ÄúInjury, poisoning, and certain other consequences of external causes‚ÄĚ, while the category with the highest proportion of incorrect coding was ‚ÄúFactors influencing health status and contact with health services‚ÄĚ.
Evaluation of the validity of the principle diagnoses and the codes recorded in the discharge summaries revealed that ‚ÄúType 2 diabetes mellitus with coma‚ÄĚ had the lowest sensitivity. This study found that around 5% of Type 2 diabetes mellitus diagnoses had no objective evidence to support them. Miscoding also occurred in 6%‚Äď7% of diabetes records.
The validity of the principal diagnoses given in the discharge summaries was low. In practice, physicians had written clinical or pathological diagnoses in the discharge summaries that differed from the medical terminology groups used in ICD-10. The coding was often incorrect, even though there were standard coding guidelines available. Some physicians did not write complete clinical information in the medical records or discharge summaries. Coders subsequently entered ICD-10 codes based on the diagnoses recorded by the physicians in the discharge summaries, but without any supporting clinical information being present in the medical records, resulting in incorrect ICD-10 codes. This is significant because, to properly code diagnoses, many coding criteria (which are detailed in the Standard Coding Guidelines) rely on supporting clinical information found in the medical records.
The category ‚ÄúSymptoms, signs, and abnormal clinical and laboratory finding, not elsewhere classified‚ÄĚ should be avoided if a physician can summarize a diagnosis at the end of a patient‚Äôs hospitalization. There were some problems with the coding of ‚ÄúInjury, poisoning, and certain other consequences of external causes‚ÄĚ, and ‚ÄúFactors influencing health status and contact with health services‚ÄĚ, in that there were incorrect principal diagnosis codings of referral treatments (e.g., follow-up care and convalescence care). A previous study found that external causes of injury were not coded in a reliable and valid manner, e.g., pedestrian injuries were often miscoded as falls [10]. Hospitals may be more likely to report diagnosis and procedural codes that will allow them to receive larger reimbursements, while some data might be ignored simply because of a lack of financial incentive for physicians to record them.
In Thailand, physicians are generally not trained in ICD-10 coding, except for physician auditors. There is a shortage of competent coders in hospitals. They come from diverse backgrounds: medical statisticians, nurses, physicians, public health staff, medical record staff, information technology staff, finance staff, accounting staff, as well as workers with only short-course coding training. There are many steps in coding processing, such as discharge summarization, completeness checking, diagnosis and procedure coding, code checking, relative weight challenging, coding reporting, and internal summary preparation and coding auditing [56].
This study found that the discharge summaries had the most coding errors. The first requirement is to understand the pathology and physiology of diseases, co-morbidities, and complications (e.g., type 2 diabetes mellitus with coma, including hyperglycemia, hypoglycemia, hyperosmolar, ketoacidosis; congestive heart failure; chronic kidney disease [stage 5]; chronic obstructive pulmonary disease with acute lower respiratory infection; and fever).
A second requirement is that unspecified diagnoses need to take consideration of the results of laboratory tests, X-rays, CT scans, and/or the scope of investigative diagnoses (e.g., for lobar pneumonia, bacterial pneumonia, acute bronchitis, gastroenteritis and colitis of infectious origin, functional dyspepsia, gastrointestinal haemorrhage, urinary tract infection, and cerebral infraction). In many cases, doctors make diagnoses without having any results of laboratory tests, X-rays, endoscopy investigations, or specimen cultures due to the non-severity of the cases or a lack of clinical manifestation, signs, and symptoms.
Finally, physicians and coders need to understand the criteria for principal diagnoses and to develop the skills and experience required to choose the correct principal diagnoses and secondary diagnoses (comorbidities and complications). Some coders did not graduate in the health field, or received only a coder-certificate or on-the-job training, so they may not understand the pathophysiology of diseases and their clinical manifestations, despite using the Standard Coding Guidelines. Many disease diagnoses were incomplete or incorrectly coded [1112131415]. The accuracy of the assessment data depends on the quality of the medical record charts as well as the skills and knowledge of the auditors and coders, even when they have undergone a training process.
In summary, the main error sources include variance in clinical knowledge, the quality of written records, the depth of coder training and experience levels, the hospital's quality-control efforts, as well as unintentional and intentional coder errors (such as misspecification, unbundling, and upcoding) [16]. Based on the findings of this study, the validity of the principal diagnoses recorded in summary and coding assessments were found to be low. Improved training would be beneficial for strategic planning and would strengthen the validity of discharge summaries and codings. Physicians should record information in discharge summaries correctly, clearly, and completely to improve coding validity, especially for the categories ‚ÄúEndocrine, nutritional, and metabolic diseases‚ÄĚ, ‚ÄúSymptoms, signs, and abnormal clinical and laboratory finding, not elsewhere classified‚ÄĚ, and ‚ÄúFactors influencing health status and contact with health services‚ÄĚ. Coders should also have a comprehensive knowledge of coding criteria and should develop the requisite skills, particularly when coding the categories ‚ÄúInjury, poisoning, and certain other consequences of external causes‚ÄĚ and ‚ÄúFactors influencing health status and contact with health services‚ÄĚ.