Auditing Knowledge toward Leveraging Organizational IQ in Healthcare Organizations
Article information
Abstract
Objectives
In this study, a knowledge audit was conducted based on organizational intelligence quotient (OIQ) principles of Iran's Ministry of Health and Medical Education (MOHME) to determine levers that can enhance OIQ in healthcare.
Methods
The mixed method study was conducted within the MOHME. The study population consisted of 15 senior managers and policymakers. A tool based on literature review and panel expert opinions was developed to perform a knowledge audit.
Results
The significant results of this auditing revealed the following: lack of defined standard processes for organizing knowledge management (KM), lack of a knowledge map, absence of a trustee to implement KM, absence of specialists to produce a knowledge map, individuals' unwillingness to share knowledge, implicitness of knowledge format, occasional nature of knowledge documentation for repeated use, lack of a mechanism to determine repetitive tasks, lack of a reward system for the formation of communities, groups and networks, non-updatedness of the available knowledge, and absence of commercial knowledge.
Conclusions
The analysis of the audit findings revealed that three levers for enhancing OIQ, including structure and process, organizational culture, and information technology must be created or modified.
I. Introduction
The development of a knowledge-sharing culture is a process of change on the way to better organizational performance. To achieve that change, an organization needs a vision of where it wants to be and an accurate picture of where it is now—that is, its current reality. A knowledge audit (KA) is one way of achieving this. KA helps organizations identify their knowledge-based assets and develop strategies to manage them [1].
Healthcare organizations are rich in intellectual capital because they have a variety of specialists, technologies, and environmental links [2]. Therefore, the proper management of these assets and the development of syntropy (the coming together of people, ideas, resources, systems, and leadership in such a way as to fully capitalize on the possibilities of each) among them can increase the organizational intelligence quotient (OIQ) and create value for these organizations. OIQ was defined as "a quantitative measure of an organization's effectiveness in information distribution, decision-making, and action based on the information." High organizational IQ can lead to the development of agile, learning, innovative, and intelligent organizations [3].
OIQ has 5 principles which are briefly defined here. External Information Awareness means the degree to which an organization has developed a deep and consistent understanding of its environment. Internal knowledge dissemination ensures that each part of the organization knows what it needs to know when it needs to know it. Continuous innovation means the reinvention of products, services, and processes, and it is a key strength of leading organizations. They generate break-through ideas that turn into market successes by promoting creativity and innovation across all functions, hierarchies, and boundaries of an organization. They also have strong actions that allow them to learn from and improve existing processes. Effective decision architecture helps decision-makers to make critical strategic decisions, without overwhelming them with tactical decisions that can and should be made by contributors at multiple levels with a perspective more appropriate for those decisions; and organizational focus refers to the avoidance of information overload and organizational complexity as well as the alignment of organizations along their strategies [3].
Numerous studies have been performed on the execution of knowledge management (KM) projects in organizations. In all these studies, there is a reference to a stage known as auditing at the beginning of KM execution in organizations [4567891011]. A KA can have multiple purposes, but the most common purpose is to provide tangible evidence of what knowledge an organization needs, where that knowledge is, how it is being used, what problems and difficulties exist, and what improvements can be made [1]. In this study, a KA was conducted based on OIQ principles of Iran's Ministry of Health and Medical Education (MOHME) to identify levers to enhance OIQ.
II. Methods
In this qualitative research, a multi-method approach including interview, structured observation, questionnaire, and workplace walkthroughs were employed. MOHME was determined as the study environment because it is the main decision-maker in the field of healthcare and medical education in Iran. The ministry has a specific mission, a specific vision, and specific goals. Moreover, its policies guide all health, treatment, and medical education centers. MOHME, with 300,000 employees, is the second largest ministry in Iran. Since the service life of most senior managers in the Iranian government agencies is short and usually associated with changes in government, changes in management staff are inevitable. Therefore, in this ministry repeatedly projects bring costs and waste resources. If managers are informed of other defined projects in their organization, they can prevent repeated projects.
The study population consisted of 15 senior managers and policymakers in such departments as the Policymaking Council, KM and Organizational Learning, International Relations, Management Development and Administrative Reform, and Statistics and IT at MOHME. To prepare the questionnaire for the KA, a review of studies on KM was done first. Then, a panel of experts was convened. For this panel, 21 experts were invited, but only 15 attended. A second panel was also convened because the experts failed to achieve any results in the first panel. The first panel met for 45 minutes, and the second panel met for 35 minutes. The experts participating in the panel were two groups. The first group included subject-matter experts, who theoretically had the necessary expertise in KM. In the other group, there were experimental experts, who had a background in KM projects. Finally, the tool was validated with a Cronbach's alpha reliability estimate of 0.91.
The tool contained 5 items on external information awareness, 5 items on internal knowledge dissemination, 5 items on continuous innovation, 14 items on effective decision architecture, 13 items on organizational focus. Data was collected by reference to the above-mentioned departments and structured interviews with senior managers. Each of the questions was measured with suitable options. For some questions, the participants could give more than one answer.
III. Results
In this KA, 60% of participants were male, and the others were female. Some 46.6% of participants were 35 to 40 years old. Also, 66.7% of managers had 6 to 9 years of working experience. Nearly 60% of them had PhD degrees in various fields, such as healthcare management, social medicine, and executive management. About 40% of them were active in the Center of Management Development and Administrative Reforms (Table 1).

Socio-demographic characteristics of study sample
As presented in Table 2, based on principle 1 (P1), KA revealed that this principle had the necessary features. Regarding principle 2 (P2), most managers did not know about the place of specialists in a certain field, and auditing based on principle 3 (P3) showed peoples' unwillingness to share knowledge; insufficiency of the existing information in the database, library, technical journals or other media for innovation; lack of a mechanism to determine repeated tasks; and lack of the organization's praise for the formation of societies, groups, and networks.
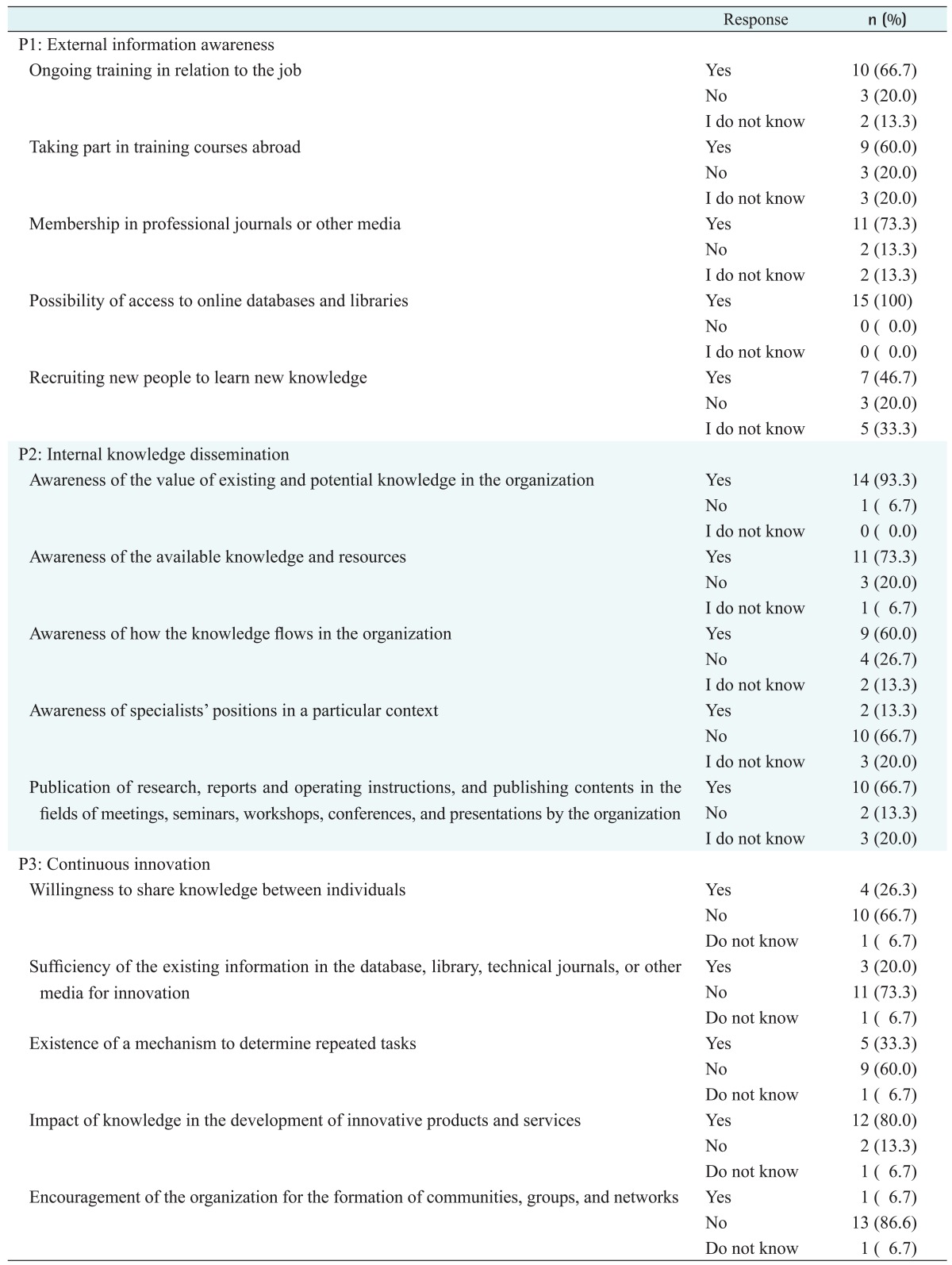
Knowledge audit based on the first, second, and third principles of organizational IQ
Table 3 reveals that, regarding P4, the use of IT is in an ideal condition, and the bottlenecks are in sections related to knowledge sharing as determination of the level of access to knowledge, outdatedness of available knowledge, establishment of private relations with specialists to achieve the required knowledge, implicitness of the knowledge format, and the occasional documentation of knowledge for reuse.
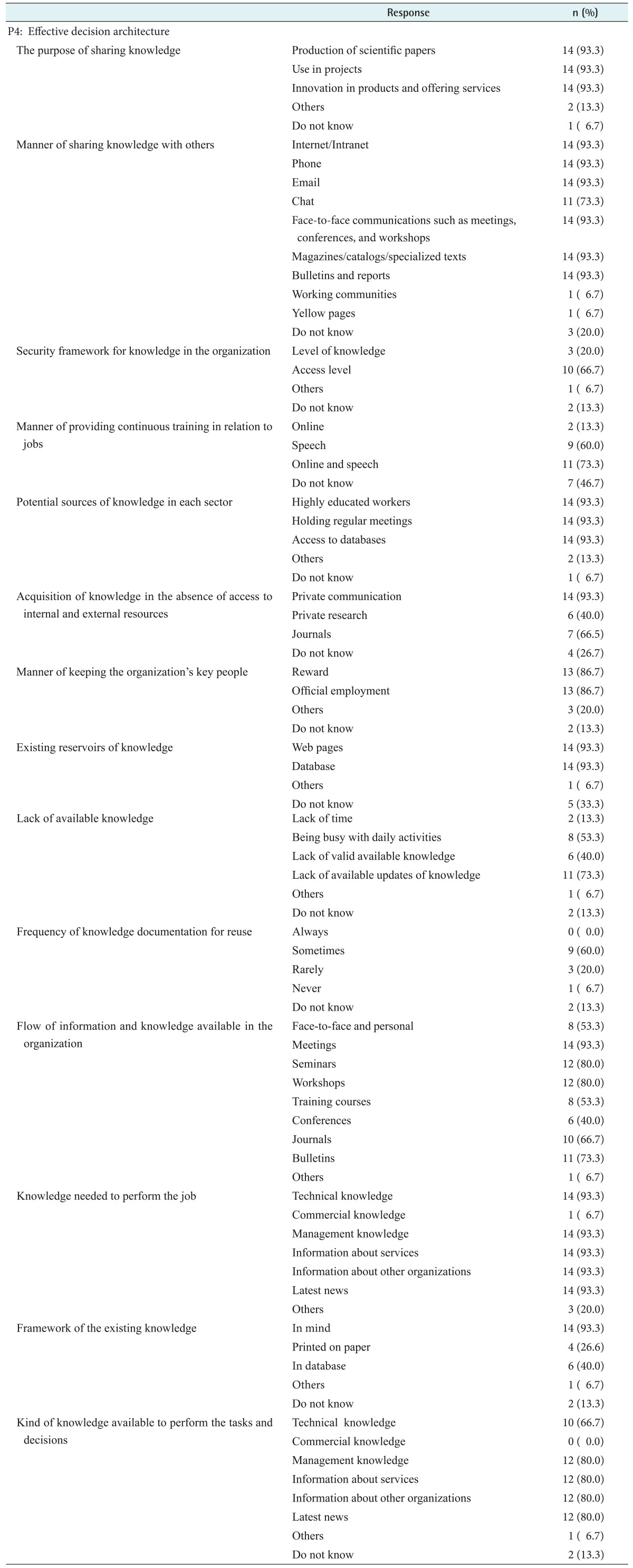
Knowledge audit based on the fourth principle of organizational IQ
As it can be seen in Table 4, regarding the P5, i.e., organizational focus, MOHME does have the necessary potentials for KM implementation, but it lacks a codified program to do so. The reason for the lack of knowledge map is the absence of a trustee for KM implementation and a specialist for knowledge map preparation, and the reason for KM problems in the organization is the absence of a suitable team for knowledge-related programs and of standard processes for organizing KM.
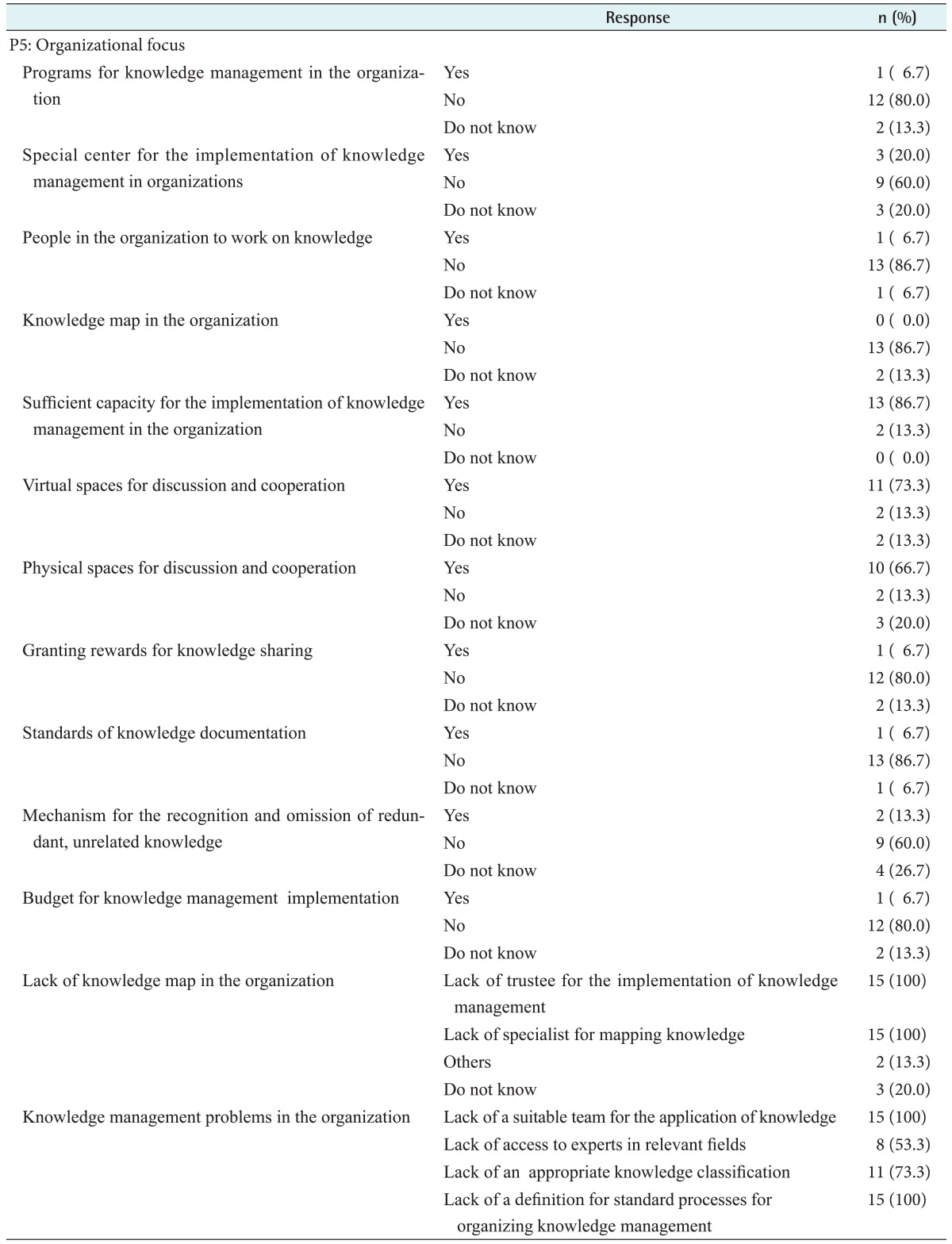
Knowledge audit based on the fifth principle of organizational IQ
IV. Discussion
To succeed in an OIQ enhancement program, the first step is to conduct a KA [1213]. In various studies [89121415161718192021222324252627282930313233], special attention has been paid to the alignment between KA and the organization's business strategies, objectives, and goals, as well as the role of IT and its effect on KM to create competitive advantage for the organization [121534]. Therefore, the first stage of auditing is allocated to knowing the organization, i.e., knowing the organization completely in terms of goals and environment, inputs and output, information sources, organizational culture, and information technology. Of course, with a systematic study of models and the various stages of KA, it can be accepted that no single model can be suitable for all organizations or under all conditions. The validity and usability of the KA model, therefore, varies according to the size, geographical region, or age of the organization [1116].
Our KA based on the five OIQ principles and its levers, revealed that despite the existence of organizational learning and a KM department in MOHME, an organizational structure for KM implementation should be designed to leverage OIQ. That is because the ministry has the potential needed for KM implementation, but lacks the structure, processes, and mechanisms needed to do so. Since the implementation of any approach basically depends on the culture of that organization, before implementing KM, its members should become informed about the effect of each member's knowledge on the improvement of performance, production of better services and products, and finally, the enhancement of public health [1835].
Based on the first principle, auditing showed that the role of specialists is not specified in a certain field—a finding which implies the necessity of creating knowledge map for the organization. Based on the fifth principle of auditing, the reason for the lack of a knowledge map is the absence of a trustee of knowledge management implementation and of a specialist to produce such a map; therefore, certain specialists should be trained in the field of KM to classify knowledge in various areas related with the affairs of the mentioned ministry, to prepare organizational knowledge maps, and to update them [1436].
In auditing, results regarding the second and third principle can be indicative of the fact that, in knowledge sharing, such concepts as rivalry, jealousy, individualism, obligation, and privacy invasion may be brought up; and for the proper management of any one of them, it is necessary to instill a culture to create a common vision aligning with the achievement of knowledge-based health and a healthy society. It is also necessary to apply idea registration and incentive mechanisms to create motivation in knowledge production and sharing. In addition, knowledge documentation and sharing should be carried out by trained individuals, and a team should be formed to update the knowledge available to managers for their sufficient use. It has also been shown in various studies that acting upon the lessons learned has not been a priority for most organizations; the needed capacity should be created, and effective mechanisms should be adopted to organize and document experiences [914172537].
On the other hand, in auditing based on the fourth principle, it was found that the use of information and communications technology (ICT) plays an important role in knowledge sharing. Although the holding of sessions in an organization is a suitable environment for top-down and bottom-up knowledge flow, a suitable IT-based communications network must be formed among members so that they can easily exchange the knowledge they need and make decisions together. The Internet and Internet-based devices play a facilitating role in the production, use, and sharing of knowledge. Thus, it is necessary to prepare the grounds needed for the application of IT because other studies have also mentioned the use of communications- and IT-based devices as a basic factor in the distribution and acquisition of knowledge. Considering auditing based on the fifth principle to achieve continuous innovation, it is necessary to have access to previous knowledge and information to avoid doing repeated tasks and to foster an environment and spirit of partnership for knowledge sharing. Therefore, communities of practice should be formed using IT for the exchange of knowledge to achieve the best practice and to facilitate relationships with scientists and local and foreign specialists, and electronic systems should be developed so that individuals can gain knowledge automatically to avoid the production of repetitive knowledge [161827].
In auditing based on the fourth principle (P4), the lack of commercial knowledge in organizations was identified. As mentioned earlier, in the OIQ leveraging process, syntropy should be created between sources of knowledge to produce for the organization the kind of knowledge that results in value creation for that organization. Now, special attention should be paid to the commercialization of knowledge on this basis. Therefore, it is necessary for an organization to consider business knowledge in addition to managerial and technical knowledge, and to publish the results of its research for other organizations of the country that can affect public health [3]. Finally, it can be concluded that the three levers for enhancing OIQ include structure and process, organizational culture, and information technology that must be created or modified.
In conclusion, the analysis of auditing findings based on OIQ principles revealed that despite the existence of a KM and organizational learning department in Iran's health ministry, an organizational structure for KM should be designed to leverage OIQ. The ministry has the necessary potential for KM, such as tangible and intangible sources and information technology, but it lacks the structure, processes, and mechanisms needed to perform it. Also, since the implementation of any approach basically depends on the culture of that organization, certain reforms should be carried out in this regard. In fact, KA in MOHME can lead to the smart management of medical centers. That is, it is possible to enhance OIQ with the proper management of intellectual capital and bring about a revolution in the country's health domain. Implications from this study could be useful for policy makers in other countries in working to achieve a high OIQ; they must perform KA to check the existing knowledge and the knowledge needed for their organizations; the knowledge resources in those organizations; the proper flow of knowledge throughout the organizations; the needs, roles, and tasks of knowledge brokers and knowledge workers in the organizations; and shareholders and stakeholders of knowledge inside or outside the organization.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.