Factors Associated with the Timeliness of Electronic Nursing Documentation
Article information
Abstract
Objectives
To investigate the factors associated with the timeliness of electronic nursing documentation using the entry time on the Electronic Medical Record (EMR) system.
Methods
As a retrospective study, data were extracted from January 1 to February 28, 2014 from a hospital EMR system and a nurses’ personnel information system. The timeliness of instances of nursing documentation was categorized into ‘timely’ or ‘untimely’ according to whether the entry time was time-stamped within the working hours during each day, evening, or night shift. Factors associated with the timeliness of the electronic nursing documentation were included in the logistic regression models as nurse- and patient-associated factors.
Results
Among 1,700,247 instances of electronic nursing documentation, 79.3% (n = 1,347,711) were completed within the working hours. Years of nursing experience, nursing shift, days of the week, patients’ age, and medical department had a statistically significant associated with the timeliness of nursing records. Nurses with experience of more than 1 year entered nursing records over 2 times more during their working hours than did less experienced nurses. During the evening and night shifts, nurses were 1.49 times and 9.19 times more likely to enter nursing documents in a timely manner, respectively, as compared to those in the day shift.
Conclusions
Nursing documentation was typically completed outside of working hours when a nurse had little experience, worked during the day shift or weekdays, and when tasks were unpredictable. This shows that new nurses need support to familiarize them with various tasks and the overall workflow.
I. Introduction
Direct nursing care includes activities that a nurse performs to assist the treatment and well-being of patients and to meet their health demands, whereas indirect nursing care includes activities such as management, documentation, and communication, which support nursing care [1]. Nursing records refers to the recording of patients’ status, the care or service provided to them, patient information collected through the nursing process, and a combination of nursing activities and professional care [2]. Nursing records are mandated and have a nonlinear, two-way feedback loop for the nursing process—assessment, diagnosis, planning, implementation, and evaluation. Similar to professional records, nursing records follow six principles (i.e., factuality, accuracy, completeness, timeliness, organization, and compliance with standards) [3].
With rapid advances in information technology, healthcare providers actively strive to implement hospital information systems, which are computerized systems that collect, process, and effectively manage the information needed for practice, research, education, and management [4]. Nursing information systems manage nursing services and resources within the hospital information system, and manage nursing tasks in which data are collected, transformed, stored, extracted, displayed, and communicated [5]. The nursing information system, as a part of an Electronic Medical Record (EMR) system, manages the standardized nursing data to perform tasks, effectively use nursing personnel, improve documentation and communication, track nursing services and outcomes, and calculate nursing fees. All these tasks are ultimately linked to improving the quality of patient care [6].
Regarding nursing documentation that is maintained on nursing information systems, one previous study found that nurses working in a university hospital stayed logged-in to the nursing information system for an average of at least 10 hours per day and generated nursing documentation of at least one line per minute in various nursing modules in the nursing information system. Specifically, tasks related to nursing diagnosis and nursing activity in a structured format were most frequently entered, with an average of 240 lines per day for each nurse [7]. In a study that analyzed nurses’ tasks, it was reported that, among indirect nursing activities, nurses spent most of their time on ‘nursing records and review’ [8]. These studies demonstrated that electronic nursing documentation is one of the essential nursing activities, and that it takes up significant nursing time.
Nurses and other health care providers aim to share information about patients and organizational functions that are accurate, timely, contemporaneous, concise, thorough, organized, and confidential [2]. Many heath care providers regard information included in records as important, but the actual recording process is often overlooked [9]. Amidst nurses’ busy schedules and the urgent demands that arise during shifts, they tend to think that documenting is sometimes a disruption of direct patient care, which leads them to engage in documentation after their shift is completed [10]. One study reported that nurses tended to get off work later than the designated time in all shifts owing to nursing documentation, which occurred 11.7% of the times on the day shift, 10.8% on the evening shift, and 6.1% on the night shift [11].
Since the implementation of electronic nursing documentation systems, studies have examined the use of standard terminologies in electronic nursing documentation [1213], and a comparative analyses of nursing records before and after the implementation of an electronic nursing documentation system was conducted [1415]. However, although a task analysis revealed that the time spent on indirect nursing care, such as documentation time, had decreased due to the use of hospital information systems [8], there were no attempts to examine the timeliness of electronic nursing documentation using the times entered in the hospital information systems. Therefore, the purpose of this study was to investigate the factors associated with the timeliness of electronic nursing documentation using entry times in the EMR system. These factors were then divided into nurse-associated and patient-associated factors.
II. Methods
1. Study Design
This retrospective study assessed nurse- and patient-associated factors that influenced the timeliness of electronic nursing documentation.
2. Study Subjects
The subjects of this study included descriptive electronic nursing documents that were entered into the EMR system of the Severance Hospital, a tertiary hospital, in Seoul, Korea. Electronic nursing records were collected from six wards (three medical and three surgical wards), pertaining to patients aged 19 years or older, admitted to the internal medicine or surgery department.
3. Study Variables
1) Timeliness of electronic nursing records
Timeliness refers to an appropriate time in which information regarding an event must be used before it loses its ability to influence the decision-making process. In addition to accuracy, contemporaneity, conciseness, organization, and confidentiality, timeliness is one of the attributes for maintaining appropriate health records [2]. In this study, we operationally defined timeliness as when a nurse enters electronic nursing documents between the beginning and end of his or her working hours in each shift: between 06:00–14:00 for the day shift, 14:00–22:00 for the evening shift, and 22:00–06:00 for the night shift. The timeliness of a nursing document was categorized as ‘timely’ or ‘untimely’ according to whether the data entry was time-stamped within the working hours.
2) Nurse-associated factors
Using the personnel information of nurses who filled out the nursing documents, we extracted the following nurse-associated factors: years of nursing experience, years of nursing experience in the current ward, and the shift worked on the date and days of the week on which the electronic nursing documentation was entered. Years of nursing experience were categorized according to Banner’s novice to expert model: up to 1 year as advanced beginner, 2–3 years as competent, 4–5 years as proficient, and more than 5 years as expert [16].
3) Patient-associated factors
Patient information included the age, sex, and medical department admitted when a nursing document was entered. In addition, we included a patient’s severity classification with 12 areas of nursing activities, for example hygiene, nutrition, education, activity, etc., in general wards at the study hospital, which was entered by the nurses daily. Then, those 12 areas were classified into a 4-grade system, ranging from 1 to 4, with 4 being the most severe [17].
4. Data Collection
After this study was approved by the Institutional Review Board of Yonsei University Health System (No. 4-2014-0903), the data were acquired for a 2-month period from January 1 to February 28, 2014. This was the period during which new nurses went through their training so that there was a very low chance of newly-graduated nurses working in the ward. We obtained these data from the EMR system and the personnel information system with the cooperation of the nursing department and the medical information office of the hospital. Electronic nursing documentation includes the care provided to patients and their reactions, and it is entered chronologically, mainly based on the nursing process, i.e., nursing diagnoses, nursing interventions, and nursing activities that are entered into the hospital EMR system.
A total of 1,994,433 lines were extracted from the combined nursing documents, including patients’ severity data and nursing personnel data. The ECMiner 2014 program [18] was used to examine the saved dates of the records, which were then compared based on the nurses’ working shift. Then years of nursing experience were calculated using the record date as a reference point. Data with errors in patient severity or omissions were excluded, which resulted in 1,700,246 lines of nursing records.
5. Data Analysis
The data were analyzed using the SAS ver. 9.4 program (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were used to examine the characteristics of nursing documents, nurses, and patients. The timeliness of nursing documentation, categorized as ‘timely’ or ‘untimely’, was used for the logistic regression analysis. The nurse- and patient-associated factors affecting the timeliness of electronic nursing documentation were included in the logistic regression models.
III. Results
1. Subjects’ Characteristics
A total of 2,171 patients had been admitted to the selected 3 medical and 3 surgical wards, where 99 nurses took care of the patients. In total, 1,700,247 electronic nursing records were extracted for the 2-month period (Table 1). The mean years of nursing experience was 6.2 years (SD, 6.3 years), and half of the nurses had more than 5 years of nursing experience. The mean age of the patients was 58.2 ± 14.5 years, and the largest age group was the 60–79 years group (45.3%). There were 1,212 men (55.8%), and 1,108 patients were treated in the surgical department (51.0%). Finally, 1,347,711 (79.3%) of the 1,700,247 documents were regarded as timely because they were entered during the working hours of the corresponding shift.

Characteristics of nurses, patients, and nursing documentation
2. Differences in the Timeliness of Electronic Nursing Documentation by Nurses’ Characteristics
Table 2 shows the differences in the timeliness of electronic nursing documentation in relation to nurses’ characteristics. Nurses with experience of one year or less created records in a significantly less timely manner (68.5%) as compared to nurses with more years of nursing experience (>80%). Regarding the difference in timeliness in relation to shifts, nurses working night shifts exhibited more timeliness (96.3%) than did those working in the evening (80.6%) and day (73.7%) shifts. There was also a statistically significant difference in the timeliness, with 77.1% occurring during weekdays and 85.7% on weekends.
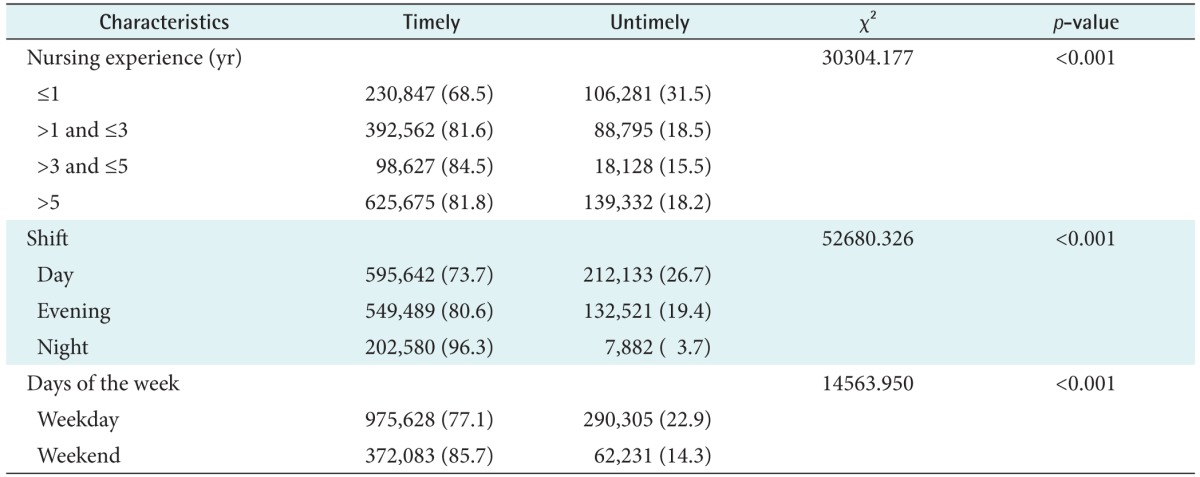
Timeliness of electronic nursing documentation by nurses’ characteristics (n = 1,700,247)
3. Differences in the Timeliness of Electronic Nursing Documentation by Patients’ Characteristics
Table 3 shows the patient characteristics and the timeliness of the electronic nursing documentation. A majority of the documents pertained to patients with grade 2 severity, and the timeliness of the records for this group was better (79.8%) than that for the documents of patients with other grades of severity. Similarly, more timely data entry occurred for patients of the surgery department (80.2%) as compared to their counterparts (78.0%).
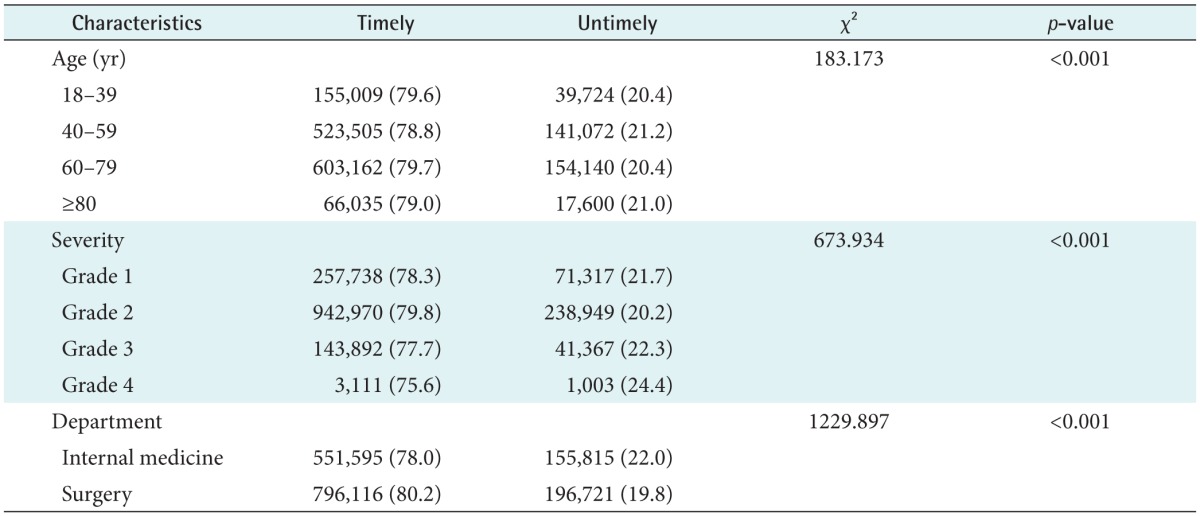
Timeliness of electronic nursing documentation by patients’ characteristics (n = 1,700,247)
4. Factors Associated with the Timeliness of Electronic Nursing Documentation
A logistic regression was performed to examine the factors associated with the timeliness of electronic nursing documentation, in which nurse-associated factors, such as years of nursing experience, shift, days of week, and patient-associated factors, such as age, severity, and medical department, were used as independent variables (Table 4). The completion of the documentation within the working hours of a shift was used as the dependent variable. The results showed that nurses with more than 1 year of nursing experience completed electronic nursing documentation two times more often during their work hours than did nurses with an experience of 1 year or less. Furthermore, the nurses entered electronic nursing documentation 1.95 times more often on weekends than they did on weekdays, and 1.49 and 9.19 times more, respectively, during evening and night shifts than those during the day shift.
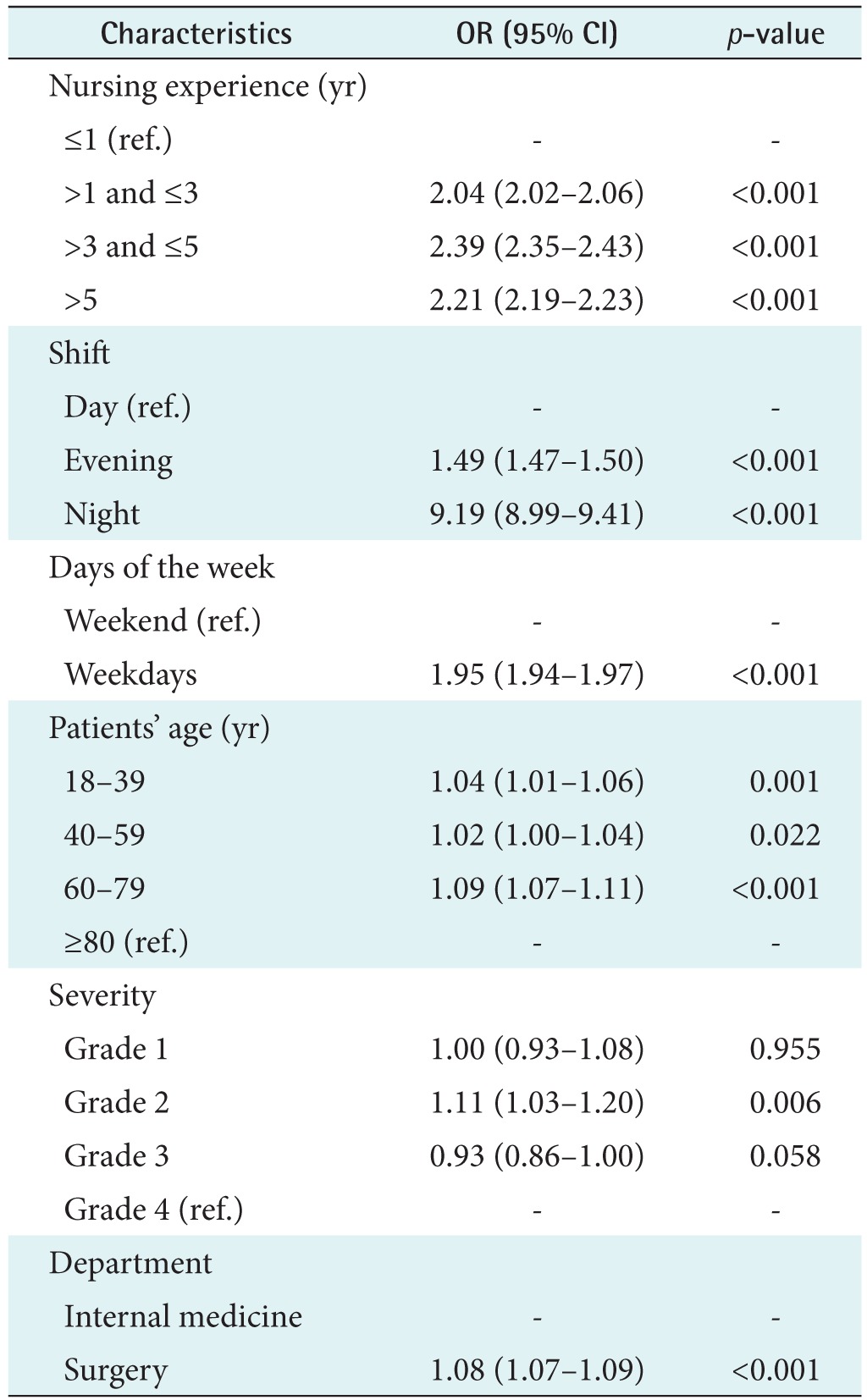
Factors associated with timeliness of electronic nursing documentation (n = 1,700,247)
In terms of patient factors, the electronic nursing documentation for patients with severity of grade 2 was entered 1.11 times more often than was that for patients with severity of grade 4, and there was no difference among the other groups. In addition, electronic nursing documentation for patients of the surgery department was completed 1.08 times more often during the working hours than for patients of the internal medicine department. In summary, nurses’ characteristics were statistically significant factors associated with the timeliness of electronic nursing documentation after adjustment for patients’ age and severity grades.
IV. Discussion
In this study, we examined factors associated with the timeliness of electronic nursing documentation using the entry time of electronic nursing documentation by nurses. Although hospital information systems and EMR systems have been implemented for a long time, to our knowledge, no study had yet analyzed the nurses’ documenting patterns.
Nursing documentation is used as an effective communication method among healthcare professionals. However, nurses often consider the documentation of these records as a burden or a task that interrupts patient care. Sufficient time and resources that can support documentation are required to produce high-quality nursing documentation [2]. Nursing activities, such as nursing problems, daily plans and goals, admission assessment, routine assessment, nursing intervention, and evaluation, appear in the system. These are diverse and recursive processes; however, the nursing information systems were often developed without sufficiently reflecting the user experience, which resulted in multiple screens, and redundant data entry required on different screens [19]. This indicates that the EMR systems’ accessibility decreases and it takes a new user a longer time to become accustomed to the system.
We observed that there was a statistically significant difference in timeliness between nurses with one year or less nursing experience and those with more years of experience, with 68.5% and more than 80% of timely documentation within the working hours, respectively. Based on the odds ratio, nurses from all other groups completed documentation within their work hours, with more experienced nurses showing timeliness two times more often than did those with 1 year or less experience. Thus, it seems that advanced beginner nurses have difficulty in getting used to the nursing information system. A study on the experience of a novice nurse in becoming an advanced beginner nurse [20] found that novice nurses experienced a sense of inadequacy because they were not accustomed to the overall workflow, systems and administrative procedures. Although this group of nurses received nursing documentation entry training during their orientation period, it is evident that they need more time to become proficient in their tasks, including nursing documentation. This shows that support is needed in order for new nurses to get familiar with their various tasks and the overall workflow. A study reported that providing a manual to encourage nurses to self-learn at their own pace resulted in increased task proficiency [21]. This indicates that various approaches are necessary until new nurses are fully accustomed to their work and environment.
Nursing shifts were a significant factor associated with timeliness, where the incidence of timely nursing documentation was 9.19 times higher in the night shift as compared to that in the day shift. Similarly, weekends also showed higher timely nursing documentation entry incidence than did weekdays. For nurses working on night shifts or weekends, fewer unpredictable incidents may have led to the higher timeliness as compared to day/evening shifts or weekdays, when there is usually more work to do, e.g., admissions and discharges, surgeries, procedures, and tests.
However, difficulties in the timeliness of electronic nursing documentation cannot be simply attributed to the volume of records alone. Upon examining the differences between departments, it was found that there were 1,023 and 1,108 fewer internal medicine department patients as compared to surgery department patients, with a record volume of 551,595 and 796,116, respectively. Yet the timeliness of nursing documentation for surgery patients was 1.08 times higher than was that for internal medicine patients. A previous study that examined the activity log data of nursing information systems [19] found that there were several repetitive nursing tasks. Such nursing tasks do not occur independently; rather, they influence one another so that nursing tasks can be carried out effectively when nurses predict which tasks will affect others. In that sense, most surgery patients have surgical treatments that are pre-planned; therefore, their nursing tasks are more predictable than are those of internal medicine patients. On the other hand, it is more difficult to predict tasks for internal medicine patients because the treatments and patient status tend to change unexpectedly.
This study had limitations in that the analysis was performed using only some wards in one hospital; thus, the findings may not be generalizable. We were unable to find differences according to the EMR systems in multiple domestic institutions that were developed with various designs and functions. Thus, further studies are needed to include data from other medical institutions to examine nurses’ recording patterns. Because we only analyzed records for adult patients in general wards, there is a need for a study using various clinical environments and patient populations as subjects, such as intensive care units and emergency rooms.
We found that nursing documents were typically completed outside of work hours when a nurse had little experience, worked during the day shift or weekdays, and when tasks were unpredictable. To implement a system that increases the timeliness of electronic nursing documentation, we must assess the characteristics of nursing tasks and analyze the nursing workflow in detail. Because no previous studies have used the entry time as was done in the present study, we will be able to assess the entry form of nursing documentation in more detail through a replication study in various environments. We also believe this will contribute to the creation of more convenient and effective entry forms in hospital information systems while maintaining the quality of nursing documentation.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.