Development of Smartphone Educational Application for Patients with Coronary Artery Disease
Article information
Abstract
Objectives
This study was conducted to develop a smartphone application (app) as an educational learning instrument for coronary artery disease (CAD) patients and to assess the users' level of satisfaction.
Methods
This methodological research involves elicited learning content for CAD patients to develop a learning instrument using the smartphone app. The app was developed according to the steps of Assessment, Design, Development, Implementation, and Evaluation, which is a systematic instructional design model. The levels of satisfaction with the developed smartphone app among 30 outpatients with CAD were assessed via a questionnaire during their visits to a cardiology outpatient department.
Results
A smartphone app 'Strong Heart' was developed through reviewing the literature associated with education for CAD patients under professional supervision and searching for medical smartphone apps that are already available. The learning contents include six main sections containing essential learning issues in managing CAD and additional information to attract the user's attention, such as patient cases and quizzes. After modification with feedback from experts, the app was finally developed and evaluated by patients who reported that they were satisfied with the usefulness of the app.
Conclusions
The developed smartphone app is available on both the iPhone App Store and the Android Play Store. Patients with CAD may utilize the app for supporting educational material without limitations of time and space.
I. Introduction
For the past decade, the prevalence for coronary artery disease (CAD) including stable angina and acute coronary syndrome (ACS) among chronic diseases has doubled from 0.8% to 1.6% in Korea [1]. With the development of a thrombolytic agent and such interventions as percutaneous transluminal coronary angioplasty and endovascular therapy, the health of patients with ACS, including acute myocardial infarction (AMI) and unstable angina pectoris, has been improving dramatically. However, 21% of 8,425 AMI patients in Korea-who were able to be tracked 12 months after discharge-reported the occurrence of adverse cardiac incidents, such as death, restenosis, and recurrence [2]. A combined approach of adhering to consistent medicine-taking and improving lifestyle habits-smoking cessation, dietary, and exercise management, as well as stress control-is effective in curbing adverse cardiac events.
Two-year follow-up observation of CAD patients after their receiving lifestyle interventions revealed that the patients who received lifestyle interventions showed an increase in physical activities, a decrease in the frequency of reperfusion therapy, and an increase in survival rates compared to those who did not [3]. According to a multi-institutional study of about 18,000 ACS patients from 41 nations, patients who continued smoking and made no improvements in diet and exercise habits were 3.8 times more likely to have recurrence of ACS or to have high incidences of mortality due to stroke compared to non-smoking patients who showed improvement in lifestyle habits [4]. Therefore, there is a need for an educational strategy for CAD patients to help them stay fit through therapeutic lifestyle changes and a need for consistent research on the effects of individualized educational interventions [5].
Many studies have been conducted to identify an effective strategy for individualized health education to enhance the knowledge and self-care compliance of CAD patients in Korea [6,7,8]. Some educational multimedia materials have been developed, such as a program using video-audio media for CAD patients [7] and an Internet-based courseware for hyperlipidemia patients [8]. Although computer-based support can help patients and their families make health-related decisions, such support is of little help to them in places where there are no computers available.
Educational programs using smartphones, netbooks, and tablet PCs have recently been employed for discharge education for chronic disease patients thanks to the increased use of smartphones. South Korea had the highest level of smartphone ownership in the world, and the smartphone penetration rate reached 79.5% in 2012. Smartphone ownership is expected to reach 88.9% in 2017 [9]. The important feature that sets smartphones apart from existing mobile phones is that the operating system installed in smartphones makes it possible to install and delete diverse applications (apps) [10]. The number of medical or health-related apps registered in the Apple App Store or in Android Google Play Store has recently been growing [11]. Education-related apps have turned out to be the third-fastest growing app category following the game and entertainment categories [12], confirming the growth of educational apps for patients or health professionals as an effective learning method. Recently, many mobile apps for health management have been developed in Korea. The developed apps are to help with weight loss or lifestyle changes, and they include a healthcare modeling for pregnant mothers [13], a weight loss program on obesity and body composition in adolescents [14], and a smartphone app promoting breast self-examination [15]. Although numerous educational apps are available in domestic and international app stores, there has been no app for the purpose of educating patients with CAD.
Patients with CAD have diverse lifestyle-related risk factors; therefore, there is a need for adherence to motivational enhancement through learning acquisition about disease management and lifestyle improvement to prevent the recurrence of CAD after discharge. In addition to face-to-face discharge education, the development of smartphone apps for CAD patients that will make self-controlled learning and repeated learning possible at home and at work is expected to increase the availability of information acquisition. With this background, this study aimed to develop an educational smartphone app as a self-directed learning tool for patients with CAD and then to evaluate user's satisfaction.
II. Methods
This study was conducted to develop an educational smartphone app for CAD patients by eliciting learning content and evaluating learners' satisfaction after the use of app.
1. Educational App Development Process
An educational smartphone app as a post-discharge tool for CAD patients was developed according to the steps of Analysis, Design, Development, Implementation, Evaluation (ADDIE), a systematic instructional design model [16] (Figure 1).

Development process of the application by the Analysis, Design, Development, Implementation, Evaluation (ADDIE) model.
1) Analysis and design phase
To determine the content and scope of the design, the authors. who are working as a research nurse in a cardiology department and a professor of cardiovascular nursing-carried out a literature review and an extensive analysis of existing educational brochures and leaflets for CAD patients. Also, we analyzed existing medical smartphone apps and had a meeting with cardiology physicians to discuss the contents. The design phase specifies learning objectives, and determines the learning scope and learner evaluation method based on the outcome of the analysis phase. Learning objectives focus on repeatedly acquiring knowledge about CAD through the use of smartphone apps as a motivational strength to expedite self-care implementation to prevent recurrence of CAD. The learning objectives of the main six sections are shown in Figure 2. Based on the outcome elicited from the analysis phase, a learning menu, consisting of main contents and sub-contents that require self-care implementation after discharge, was created (Figure 3).

Learning objectives of six main sections.

Composition of main menu including learning issues.
2) Development phase
Based on the learning objectives and structure determined in the analysis and design phase, an educational app was developed. The learning content was organized after consideration of the objectives and scope of learning based on the flow chart of the learning menu, and the first version of an educational app was developed by a professional Web producer. All content was created in a way that can be viewed comfortably by allowing users to enlarge and reduce the font size on the screen. With several consultations on the adequacy of the first version of the app, and after the revision by cardiology physicians and staff nurses, the final version of the app, the "Strong Heart" educational app was finally developed.
3) Implementation and evaluation phase
The appropriateness of the program was determined by assessing the effectiveness and efficiency of the program in the implementation and evaluation phases. The "Strong Heart" app was developed to run in both the iPhone and Android phone environments. A total of 30 CAD patients who visited to the cardiology outpatient department at Chonnam National University Hospital (CNUH) were asked to use the developed app; their feedback was received through responses to the satisfaction questionnaire. The questionnaire regarding learners' satisfaction was used after modification and complementing of items that were used in the research conducted by Kim and Hwang [17] to evaluate the level of satisfaction with multimedia learning content. The evaluation questionnaire included 17 items evaluated using a five-point Likert scale on the composition of the app, on the design and layout of the app, and the app usefulness. Cronbach's α for the reliability of the scale was 0.95 in this study.
III. Results
1. Development of an Educational Smartphone App
The developed "Strong Heart" smartphone app was designed to be user-friendly. Touching the startup screen makes the main menu appear; once the startup screen disappears, the six main learning sections-about CAD, daily life management, risk factors, drug management, dietary management, and exercise management-appear on the screen. Also, five icons for additional information to attract learners' attention and to strengthen their motivation-statistics, real patient cases, personal risk of developing CAD, precaution tips, and self-tests-appear at the bottom of the main screen. The statistics icon allows users to view various domestic and international cardiovascular-related statistics through images; the real patient cases icon allows users to recognize what to do when symptoms appear by including cases, such as middle-aged men and women, older adults, and patients with recurrent CAD; the personal risk of developing CAD icon allows users to look at the figures resulting from checking the incidence risk of CVD for the past 10 years, the calculation formula of obesity, assessment of lifestyle habits, and assessment of the degree of dependency of nicotine; the precaution tips menu allows users to look at precautions for hypertension, diabetes and cardiovascular disease; and the self-tests menu allows users to take quizzes. The startup screen and home menu, and the contents of the main menu are shown in Figures 4 and 5.

The start-up screen and home menu of the application.

Main six sections and additional information icons of the application.
The "Strong Heart" smartphone app was designed using the color red, symbolizing the heart as a primary color; the app was designed to attract users' interest by displaying graphic images of the heart and the images of family and healthcare professionals on the main screen.
Specifics about environments to run the "Strong Heart" smartphone app system may be summarized as follows. The iOS-based development environment used Mac OSX Lion and 2.4 GHz dual Intel Core i5 processor. The development tools were XCode 4.3 and iPhone Software Development Kit (SDK) 5. Testing of the app system was conducted with an iPhone simulator, and the app system was finally and successfully run on an iPhone. The Android-based development environment used a Windows environment that had a built-in Java SE Development Kit (JDK) 7. The development tools were Eclipse 3.8 and Android SDK 2.3. Testing of the app system was conducted with an Android Virtual Device, and the final version of the app system was run on the Galaxy S2.
2. Learner's Satisfaction
To evaluate app users' satisfaction, CAD patients were asked to use the developed "Strong Heart" and then assess their subjective level of satisfaction to identify the appropriateness and usefulness of the app. A self-reported questionnaire was distributed to 30 CAD patients who visited the outpatient department of cardiology at CNUH from October to November 2011. The mean age of learners was 48.9 ± 9.7 years (range, 31-67 years), and women accounted for 20%; 46.7% did not finish high school; 53% were professionals, and the rest were service workers, civil servants, or technical workers. About 85%-95% of the learners answered that they were satisfied with the composition, design, layout, and usefulness of the app. However, in the subjective item, they said that the touch screen of "Strong Heart" was too narrow and requested to shorten the length of content. Based on their feedback, the app was slightly modified. The mean values of learner satisfaction according to three domains with the smartphone app are shown in Table 1.
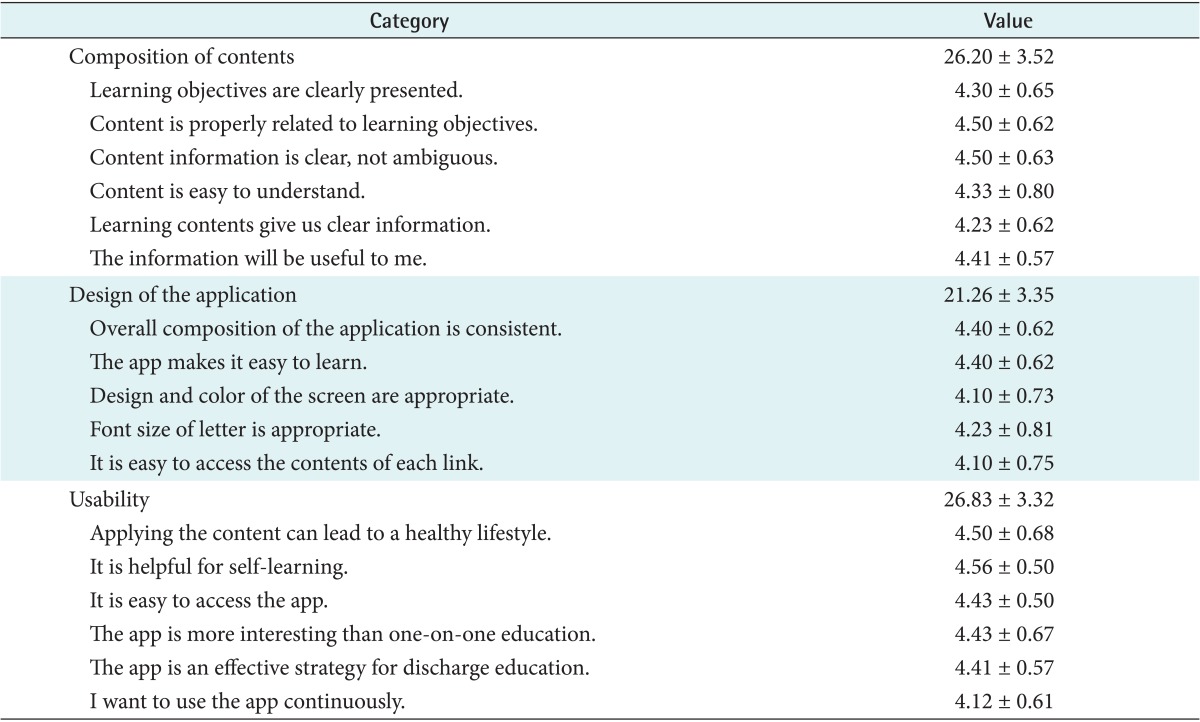
User's satisfaction on "Strong Heart" application (n = 30)
IV. Discussion
The purpose of developing an educational app for CAD patients was to create learning materials that could be accessed through smartphones as an educational strategy designed to provide treatment knowledge and nursing-related information to enhance patients' self-care implementation after discharge.
The most difficult part of the process of developing an educational smartphone app for CAD patients was determining the scope and structure of learning areas. In this study, the areas and the scope of learning were determined through interviews with cardiovascular coordinating nurses and CVD patients, and through the analysis of existing educational brochures and leaflets. The 'Strong Heart' smartphone app developed for this study stores a much larger amount of learning contents than previously developed apps. Because smartphones possess the capability to install large amounts of learning contents, we tried to include as much content as possible in the design phase, but we had to reduce the amount of contents that took a long time to load. The issue was finding the best length of apps in terms of increasing the efficacy of user's self-learning. Therefore, in future educational apps, it is necessary to consider the amount of learning content to enhance their effectiveness; further research is needed on the effect of the amount of learning content accessible from smartphone apps.
To grab the learners' attention and to motivate learners, we contained diverse animations as well as many photos and pictures. We did not include videos in the app because the app producer suggested that videos make it impossible to download due to the smartphone app capacity, and that users can experience limited connectivity problems in No Wi-Fi zones. We also had to consider situations in which excessive fees can be charged because the targeted age group to use the 'Strong Heart' app consists of middle-aged people in their 40s and 50s who use a flat fee service rather than younger people who enjoy unlimited downloads for a monthly fee.
Compared with the benefits of the existing Internet-based multimedia educational programs, the benefits of educational materials using smartphone apps are that they allow users to have an instant access to educational data and to enjoy the freedom of mobility in places where there are no computers available at any time learners need them. In a hectic ward environment, there is not sufficient time to provide education to patients on diverse risk factors with information to prevent recurrence of disease after discharge. Therefore, the "Strong Heart" smartphone app, which was developed to address such issues, will play an important role as a private electronic textbook for CAD patients. In particular, the "Strong Heart" app allows users of all ages to increase and decrease the font sizes with two icons (+, -). However, a large amount of learning menus and contents are contained in the app; as a result, some users may find it difficult to maintain learning motivation. Therefore, it is imperative to present the key content in an easily accessible and entertaining way for older adults with CAD, who are often inept smartphone users.
As for the "Strong Heart" app, icons like patient cases, personal risk, precaution tips, and self-tests were displayed at the bottom of the startup screen to enhance users' curiosity and learning motivation. Such menus set the "Strong Heart" app apart from existing smartphone apps that contain only topic-related knowledge contents. Future research should focus on expanding the user base to high-risk groups as well as CAD patients by developing a menu with a high potential for usability and by enhancing motivation of knowledge acquisition and effectiveness of education.
As for educational apps, our findings are similar with those of a study on the development of smartphone and tablet self-management apps for asthma [18]. Aside from this, to estimate the 10-year and lifetime risk of heart attack and ischemic stroke, a risk estimator using a mobile and Web version of the Excel-based calculator was released by the American College of Cardiology/American Heart Association Cardiovascular Risk Guideline [19]. In particular, another study showed that the use of smartphone app led to behavior changes and increased breast self-examination in females younger than 30 years [15]. Self-directed learning through smartphone apps can be seen as an extended nursing intervention because such learning makes it possible for patients to make behavioral changes, such as self-care implementation or lifestyle improvements, which is the greatest advantage of the present study. At a time when smartphones are popular and the market for mobile devices is growing rapidly, there is a need for the development of diverse apps related to CAD to help establish mobile education as a new form of learning.
The learner satisfaction survey of the "Strong Heart" smartphone app revealed high levels of satisfaction among patients who visited the hospital for outpatient treatment after discharge because of their intellectual curiosity about a new method of education. They showed high satisfaction with the content, design, and usability of the program; therefore, it is expected that nurses will use the smartphone app educationally for discharged CAD patients. However, only a small number of patients participated in the survey. In addition, they rated the smartphone app with a focus on the whole design without having full knowledge of the entire contents; therefore, there is a need for future surveys aimed at expanding the number of participants and focusing in detail on the learning content. Also, the focus of the present study on the development of a smartphone app has not successfully measured the effectiveness of the app. Therefore, further research should test the effectiveness of learning, and it should focus on the comparison of the effectiveness between face-to-face education and the "Strong Heart" app-based education for CAD patients. Also, there is a need for testing aimed at determining whether a combination of face-to-face education and the app-based self-directed learning rather than monotonous discharge education could enhance patients' self-care implementation. Moreover, app-based self-directed learning will be established as a nursing intervention strategy to improve the effectiveness of follow-up management after discharge. The present study has great significance, in that it tried to explore the roles of extended follow-up nursing care to enhance the knowledge and self-care implementation of CVD patients through the development of an educational smartphone app.
There were some limitations of this study. The creation of learning content for people of all ages led to large amounts of learning content, which in turn made it difficult to measure the degree of learning satisfaction and effectiveness broadly. Based on the results of this study, the following further directions for research are suggested: the development of an app including video-contained graphics that can evoke user interest, and of a simplified app with reduced contents and scope to increase the use of app among growing elderly patients with CAD. In addition, a quasi-experimental study needs to be conducted to examine the effectiveness of the use of the app in patients or high-risk group for CAD.
Acknowledgments
We thank the physicians and nursing staffs of cardiology department at Chonnam National University Hospital.
Notes
No potential conflict of interest relevant to this article was reported.