I. Introduction
'Tailoring' is the key concept of computer-tailored intervention. It is defined as any combination of information and behavior change strategies intended to reach a specific person, based on characteristics that are unique to that person, related to an outcome of interest, and derived from an individual assessment [1]. Computer-tailored interventions provide respondents with personalized feedback about their present health behavior or behavioral determinants. They provide personalized suggestions intended to change behaviors that may be potentially health threatening, and to maintain behaviors that are regarded as beneficial for health [2].
A tailored intervention can provide advantages of flexibility in time and space [3], and in addition can increase a learner's satisfaction and concentration. It can also efficiently promote behavioral change intention and recognition, and the self-motivation of the learner, since it includes less unnecessary information than non-customized intervention does [4,5,6].
In the case of total hip replacement surgery, tailored intervention is needed to ensure consistent education about rehabilitation and positions that should be avoided in the future, and exercises appropriate to recovery stages after surgery, and to lead to successful outcomes. Risk factors that may possibly occur after surgery must also be considered, including complications, infection or dislocation. The condition of each patient with total hip replacement can differ, for example, obesity before surgery, a history of hip replacement, rheumatoid arthritis with related steroid therapy, or medication for diabetes mellitus (DM). Consequently the educational content should be specific to each patient and differently focused depending on the individual characteristics of each patient [7,8,9,10,11].
Educating patients of preoperative phase without considering individual needs is not sufficient to improve postoperative outcomes [12]. Good comprehension and learning are usually achieved after applying print, computer animation based or multimedia-based teaching aides [13]. Nonetheless, there have been few studies that have considered tailored programs based on the individual's needs or characteristics, and utilizing information technology, such as the Web and computer as educational materials. Therefore, this study is aimed at developing a computer-tailored education program that can promote self-care for patients with total hip replacement based on the individual's health status and characteristics.
II. Methods
III. Results
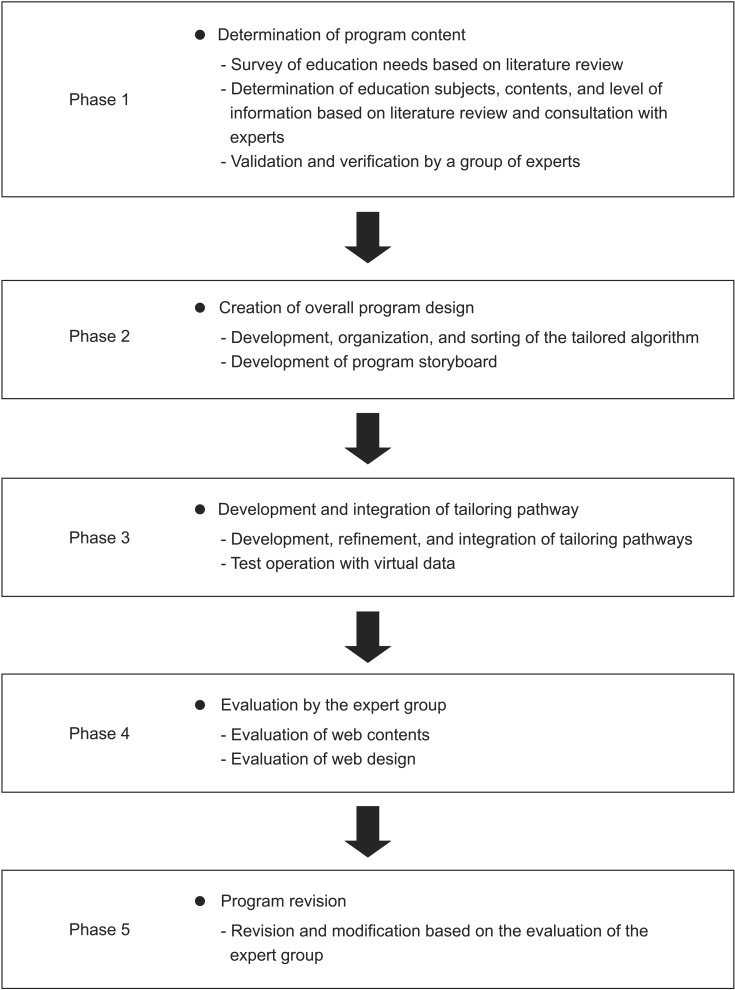
1. Phase 1: Determination of Program Content
Program content was based on three approaches: 1) literature review retrieved from 'PubMed' and 'RISS'; 2) clinical consultation with the orthopedic department of Hanyang University Medical Center in Seoul regarding nursing procedures and exercises of pre and post operation; and 3) search of information or educational materials available for the general public related to hip replacement from the websites 'National Institute of Arthritis and Musculoskeletal and Skin Diseases' and 'Medline Plus'. Finally, a total of six content categories were determined: explanation of hip replacement surgery, preoperative care, postoperative care, exercises after operation, rehabilitation and cautions in daily life.
Furthermore, we selected the tailored information, the range, topics, and depth which were to be differentiated and emphasized according to the patient's individual characteristics, for each of the contents. Also, questions were determined to categorize groups of patients and possible responses to them. An evaluation was subsequently conducted by a group of experts who was composed to two orthopedic physicians, seven nurses in orthopedics and three professors in the nursing department. Also, in order to identify how well user understand the program, quizzes were developed and displayed to users at in the middle and the end of the education program.
2. Phase 2: Creation of Overall Program Design
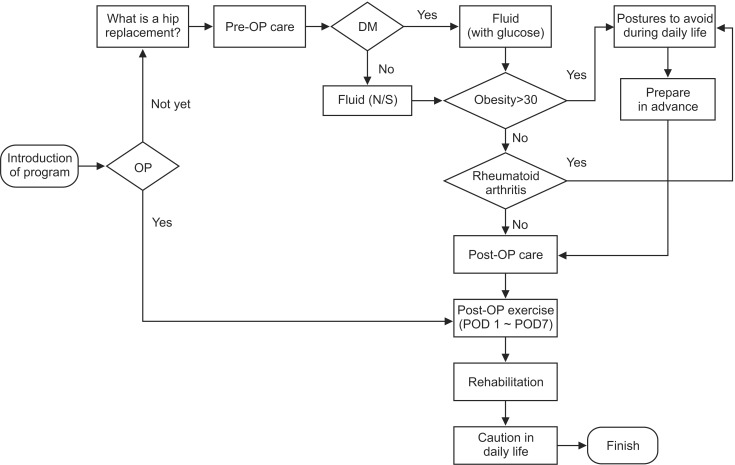
Based on the data derived from Phase 1, a storyboard was designed. For tailored information, we first determined what content would be linked to the questions and possible responses that had been developed in the previous phase, and their directions. The algorithms were integrated and revised according to comments from the expert group of two physicians in orthopedics, two nurses in orthopedics, and one professor in the nursing department (Figure 2). As a results, algorithms were subsequently made up of 'if-then' statements to sort each individual's condition and characteristics, such as 'obesity more than BMI 30 kg/m2', 'past history of rheumatoid arthritis', and 'individual health conditions on DM'. Based on the algorithms, a detailed scenario was developed and each intervention was designed to interact with the contents, as well as graphics and the display screen. Based on the functional factors of the display design suggested by a previous study [14], a display screen was designed to promote continuous motivation and effective self-directed learning using the process of Web based teaching and learning which considered the users' age and level of knowledge.
3. Phase 3: Development and Integration of Tailoring Pathway
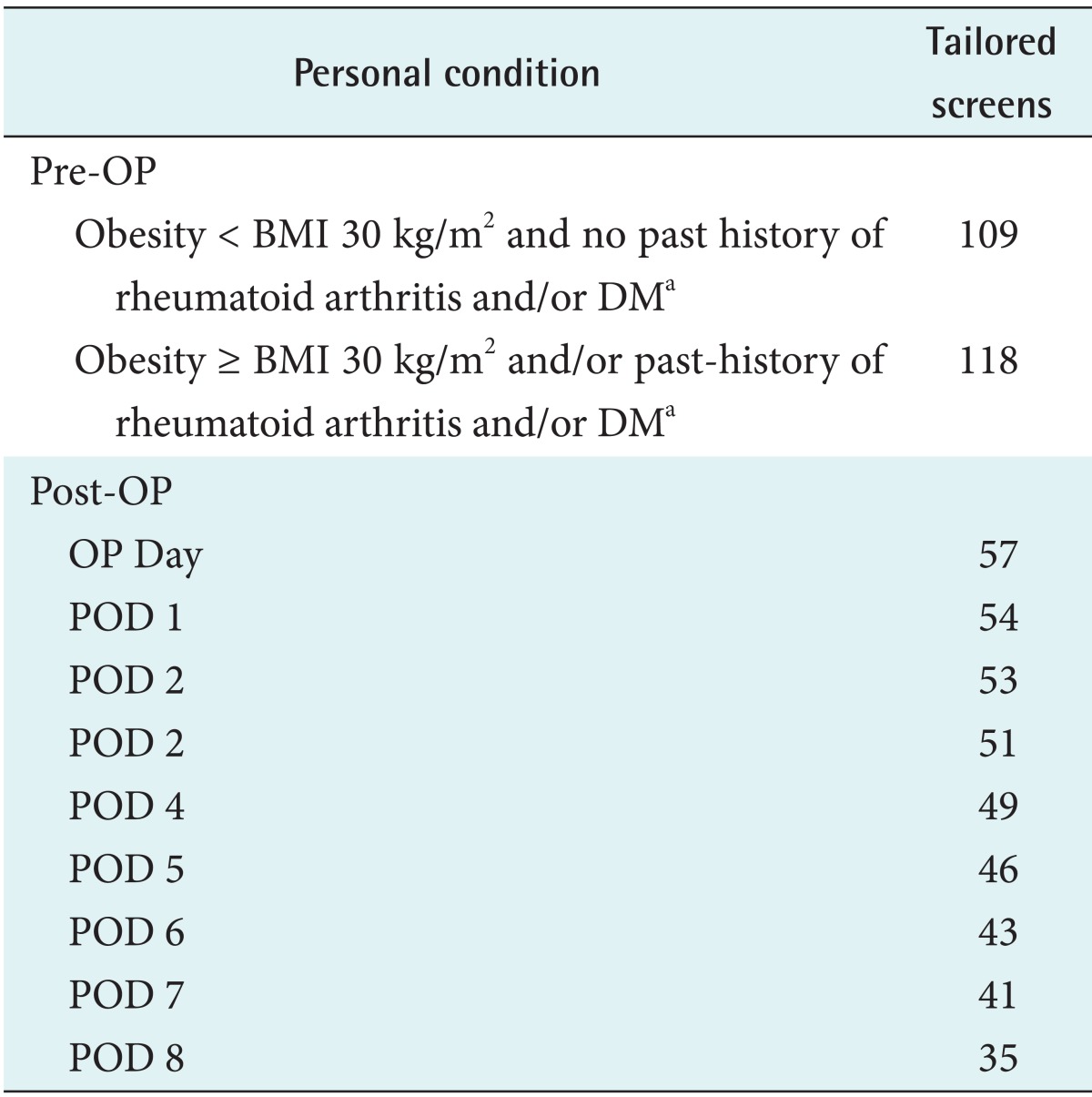
Based on the tailored direction and storyboard, the program was developed and incorporated on the Web. Except for the initial screen, the website was developed to provide different configurations of tailored display and contents depending on each individual's health status and characteristics (Table 1). In order to determine and apply the tailored directions, a survey banner for questions was located on the introduction page of the site. Then, we designed the program that all subjects have to answer these questionnaires before beginning the education, and the program based on their answer provided them with appropriate information. The questionnaire included such as the sex, age, height, weight, history related on operation, and underlying diseases (DM, rheumatoid arthritis, and so forth).
Additionally, the site operator, 'Education Team of Hip Replacement in a University', was specified on the bottom of the program, and a screen for the site developer with their contact information was also added, as well as a reference to statistics or videos, to provide credit for the information. In addition, the revision date was indicated, and information about domestic and international websites regarding hip replacement surgery was provided from the screens of useful sites. And we tested the program inputting virtual data, we corrected some typos including terms for consistency.
4. Phase 4: Evaluation by the Expert Group
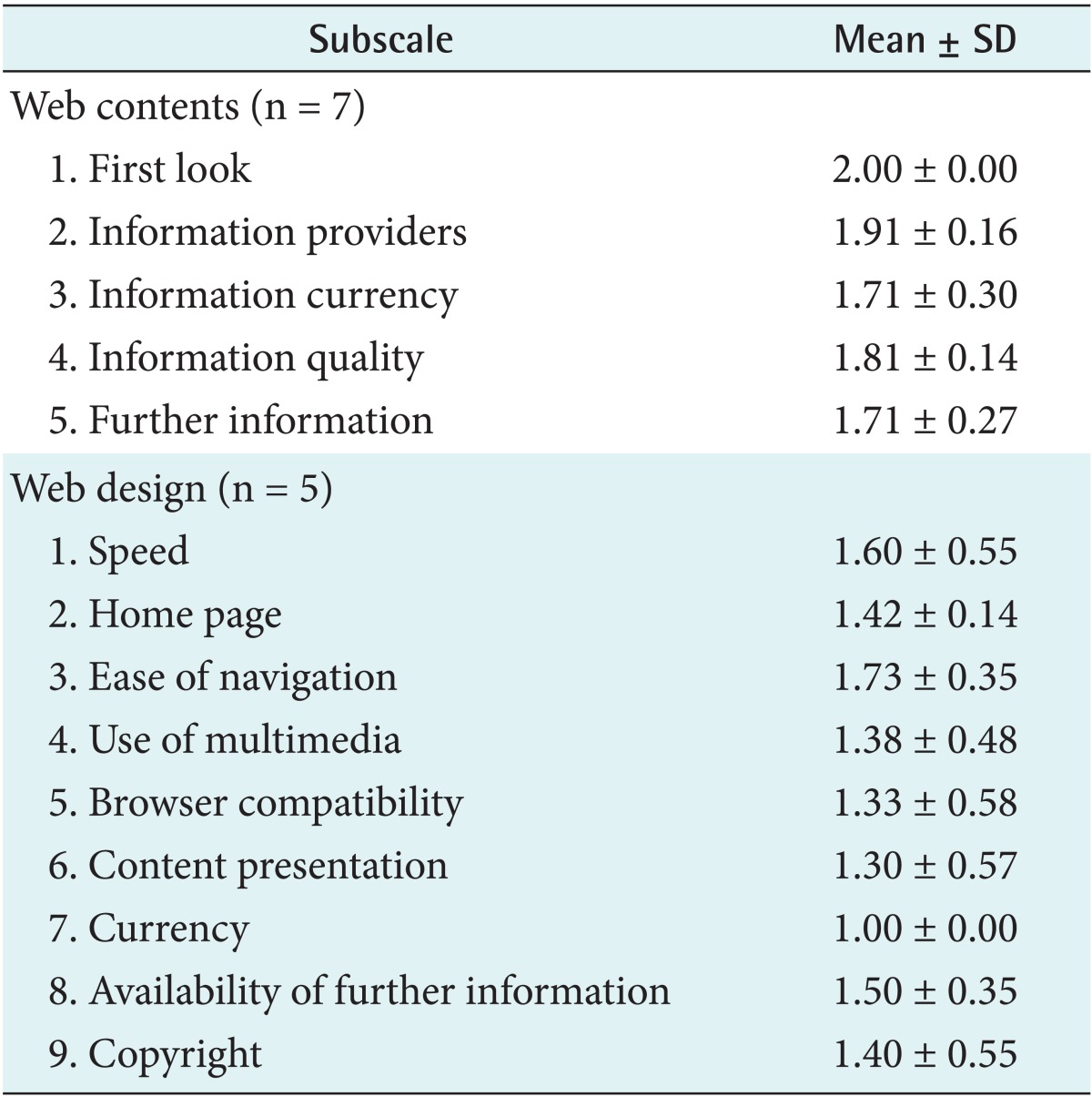
The expert group evaluated two categories: Web contents and Web design. The collected data was analyzed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA).
The clinical area of the Web contents was evaluated by one physician in orthopedics, three nurses in orthopedics and three professors in the nursing department. For the evaluation, we revised and modified a 'CyberGuide Ratings for Content Evaluation' form provided by CyberBee [15]. The reliability of the tool, Kuder-Richardson was 0.719 and intraclass correlation (ICC) was 0.741. The contents of the evaluation included five sub-sections (a total of 26 questions) and with an additional question for site rating, and a feedback section for program improvement. And the results are shown on Table 2. The result was that the item, 'first look', received a perfect score 2.0/2.0, and all items received a score of over 1.70/2.0 (Table 2). And six out of 7 experts answered 'very useful and recommendable site' and the other answered 'the site could be referenced if necessary'.
Feedback from the experts included the following comments: 'aesthetic improvement is necessary to draw more attention from learners', 'consideration of more various variables and needs to expand new questions for further tailoring', 'information on related sites and references is necessary', 'concern about the Internet accessibility of hip replacement patients considering their typical age', 'correction of typos', and 'insertion of information that the range of possible exercises are different with diseases'.
The expert group in the Web design evaluation consisted of four professional Web program developers and one researcher majoring in education engineering. For the evaluation, we revised and modified a 'CyberGuide Ratings for Web Site Design' provided by CyberBee [16].
The reliability with Kuder-Richardson was 0.720 and ICC was 0.720. The contents of the evaluation included nine sub-sections (a total of 31 questions) with an additional question for site rating, and a feedback section for program improvement. And the results are shown on Table 2. On the evaluation of the website rating, all five experts answered 'useful but aesthetic improvement required'.
Feedback from the experts included 'testing using various Web browsers and conditions is necessary', 'need to consist of more dynamic screens', 'lack of aesthetic aspect', 'too many unnecessary pop-ups', 'utilize function of Web based email to contact the site operator instead of MS Outlook', 'providing information on hospital related hip replacement surgery', 'need to filter inaccurate data', and 'correction of typos'.
The most highly scored sub-items from the both Web content and Web design experts evaluation were 'offering clear goal', 'identifying target learner', 'introducing site operator and providing contact information, such as e-mail or telephone number', 'indicating latest revised date', 'designing screen considering the level of learners', 'providing external site link and adequate functionality', 'composition of self-control by learners', 'simple usage', 'consist of program same form', and 'easiness of site navigation'.
5. Phase 5: Program Revision
Revisions based on the evaluations were comprehensively incorporated and reflected in the program. Revisions and modifications were made from May 19 to May 23, 2010 (Figure 3).
IV. Discussion
The composition of this program was determined according to the outcomes of previous studies regarding website development [17,18,19,20,21], and the contents were based on a literature review and educational materials from sources actually using in the clinical area. Because of this process based on literature, it was possible to obtain high scores of 1.81±0.14 from the Web-contents evaluation of the expert group in the section 'Information quality'.
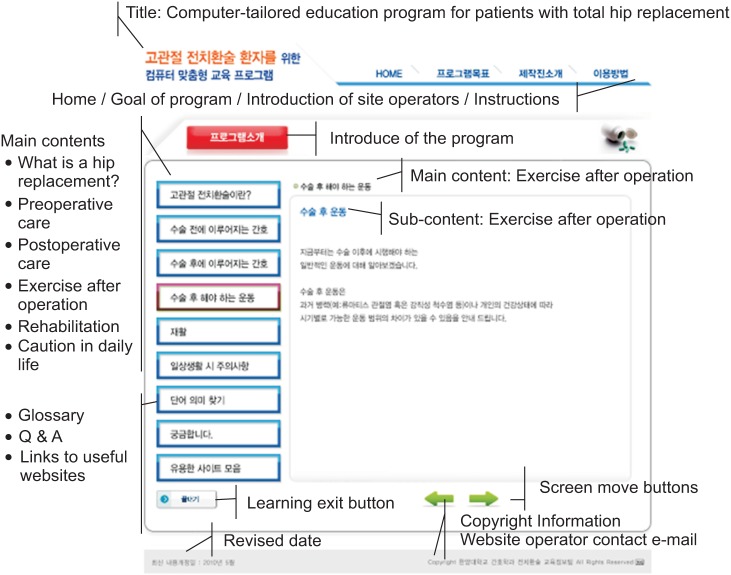
Previous studies have indicated that education using various methodologies had increased the self-efficacy and knowledge of learners [13,22]. Based on these studies, animations and flash were inserted to explain the content that focused on physical activities, such as 'how to exercise' and 'how to sit'. Videos were used to explain content focused on information regarding diseases such as arthritis. Furthermore, a feature called 'Searching the definition of words' was added to identify the meaning of 14 medical words that were frequently encountered, such as 'isometric contraction', 'quadriceps muscle of thigh', 'abrasion', 'muscular strength', etc. (Figure 4). It is expected that these features can help a learner more fully and easily understand the contents developed in the previous studies [14,17,18,19,20]. The program was designed to include an open 'Q&A' section that would allow users to contact the site operator at any time, and an emailing icon for those who wanted their questions to be private.
In designing a Web-based teaching-learning system focused on the learner, screen design is important to ensure that the learner finds the unfamiliar and new teaching-learning system friendly and easy to use. These qualities can promote learner attention, sustainable learning and self-motivated learning greatly [23]. Based on the results of the previous studies [23,24], the study aimed to design the screen to be as simple as possible, considering that the major population of hip replacements are generally over 55 years of age. This primarily involved establishing the form of the user-interface. As a result, 1) the site title was located on the upper left corner of the screen, 2) six main contents menus were vertically aligned on the left of the screen, 3) the contents display screen was placed in the center of the screen, and 4) the button to move the screen, the learning exit button, the information about the website operator and the revised date were allocated. This arrangement helps users to more easily move to other contents or menus whenever they want, and to promote easy navigation, which is in line with the findings from the previous studies [25], specifically, that people aged over 60 prefer the vertical menu configuration (Figure 4).
Additionally, the menu, including the current learning content was shown in a different color that was contrasted with the color of other sections, to make it easier to recognize the location of the learning content. Also, on the upper left of the contents display screen, the title of the content and sub-content was shown, for example 'Nursing after surgery' and 'Exercise after surgery', enabling the learner to quickly recognize the location of the learning content. These features can solve a main problem, namely, being 'Lost' [25], in which aged people are often unable to find their location on a website. The item 'how to use', which explains the website's functions and each component on the screen, was added and fixed with one of the menus on the top of the screen so that learners could check it whenever they were not sure.
This study had a limitation that the evaluation was performed by experts, not by target population, however, the results of evaluation in the Web content was shown that program content was reliable. And, the evaluators indicated that the program was presented the goal, target learner, information of site developer and operator, and provided various functions to help self-learning, such as 'service of email link to contact site operator', 'Q&A', 'information of external site links', 'searching the definition of words'. These results are consistent with the findings from the previous studies which evaluated a medical information website [14,17,18,19,20]. The contents of this program were carefully selected and fully operated by professional medical personnel. These findings are in line with the result of the previous study [26] that the development of contents by needs of professional medical personnel is more reliable, in aspects of management and quality of information, than others provided through a variety of media.
One of the feedback from the expert group was 'the improvement of aesthetic appearance is needed to promote the interest of learners'. In that regard, there were almost no previous studies for concerning the screen design of a website for medical information to users over 50 years old, the target population of our study. We can recommend conducting a study on the effectiveness of adding a section on Web design to this program, to identify the factors needed to modify aesthetic or visual aspects. Also, further study needs to consider a wider number of variables than those suggested in the tailored-condition in our study.
Another opinion concerned the 'age' of the target population. The main population of hip replacement is aged, and we have to determine whether they are able and willing to access Internet. To accomplish this, we can consider social environments, such as the following: age using Internet may be broadening, becoming younger and older, because of the continuing propagation of Internet, and the variety of user class [24]. The proportion of Internet users aged 50-59 years old has been 80.3%, and is increasing, by 20.2% compared with the previous year [27]. Business opportunities in the medical field focusing on the wellness and health of the aged are growing. We recommend that further studies should be focused on the development of Web interface designs for older ages to access easily and use Internet.
In the Web design evaluation, 'currency' was ranked the lowest. We think that the reason was the sub-item of 'currency', which was 'periodic deletion of outdated contents'. All experts answered this as 'not able to evaluate' because the development and revised date of this program was April 2010 and it could not be reflected in their evaluation. On the site rating, all five experts answered 'useful site but the aesthetic improvement required' which is similar to the results for the sub-sections of 'homepage'. In that case, 'user can immediately respond to the location of the content being learned' and 'the composition of screen is reflected aesthetic considering ages of user and increased readability' were scored low. However, this is contrary to the result of the Web content evaluation for the sub-section 'information quality', such as 'the site content is designed to consider the level of user promoting effect of learning', which was the highest score among the items. In addition, the program was deliberately designed in the simplest format, based on the literature review, including screen design and a vertical menu configuration, a font size of 20 point, single content on a screen not requiring scrolling, and the provision of site navigation with three routes, which are all features in line with previous studies [24,25,28].
We believe that the difference between the results for Web design evaluation, Web contents evaluation and the previous studies is occurred because the experts for Web design, as compared with the experts for Web content, were less familiar with the medical information and background about hip replacement and its target population. In addition, the average age of the expert for Web design was 39.8±03.42, thus they would not be as likely to find the font size, menu configuration and the font preferable because the program is aimed at older ages. This result shows that further studies related to the evaluation of Web contents by experts should consider to provide them with orientation regarding the age of target population and the medical background beforehand. Based on the results of the Web evaluation, it was clear that the program was designed to fit the target population and the information on the program was reliable, and it lead to the satisfaction of the learner.
This study developed a computer-tailored education program to provide information tailored to an individual's specific health status and characteristics using animation, video and flash, considering the age of target population. We believe that this Web-based program can repeatedly provide the same level of education, in any convenient time and space, increase user recall, and offer step by step education before and after the operation.