I. Introduction
The use of information systems in healthcare-with applications like medical records, order entry, guidelines and other types of decision support, medical knowledge provision and imaging-is steadily increasing. These information systems are usually implemented and maintained by technically orientated personnel (with a computer science background) having limited insight in the problems of medical practice. Health informaticians are not only educated to carry out research in health informatics, because of their education they are also able to function as intermediaries between the technical personnel on the one side and physicians and nurses on the other. In addition they can be support the medical staff in defining the requirements for new applications and can also be involved in the design and development of systems.
Also Musen distinguishes between computer science and health informatics: '(health) informatics is not the application of computer science, image processing, and statistics to a particular domain. Rather, (health) informatics is a primary field of study that may be targeted toward a wide variety of disciplines (health care and the life sciences being particularly important). What sets informatics apart from computer science and from other potentially confluent fields is a matter of priorities: ours is the discipline that cares about the content' [1].
There is an increasing need for health informaticians [2] and an increasing number of health informatics programs deliver graduates with different kinds of expertise.
The Recommendations on Education in Biomedical and Health Informatics [3] of the International Medical Informatics Association (IMIA) define the knowledge and skills necessary for creating different types of health informaticians. Educational institutions use these recommendations when defining the contents of their health informatics curricula. In doing so, they also have to take the needs of the labor market into account in order to endow students with employable skill sets.
Because of the growing internationalization of education-as is apparent from the increasing cross-border student and professional mobility, especially in Europe, but also elsewhere-the quality of a higher education institution affects its international status and therefore its attractiveness for students. Quality has become so important that the ranking of educational institutions has become a huge business. Universities, for example, are assessed and ranked in the Times Higher Education World University Rankings, powered by Thomson Reuter. It is stated that 13 carefully calibrated performance indicators are used to compare the universities.
However, the ranking process used by the media is often criticized. Most countries now have a national quality assurance system, but these systems are still diverse and of uneven quality. Current practices regarding quality assurance in tertiary education in the Organisation for Economic Co-operation and Development (OECD) countries have been discussed by Kis [4].
Quality is a fuzzy concept that needs to be made operational. For the educational sector quality can among others be defined in terms of fitness for purpose. Fitness for purpose relates the output of the program to its purpose as defined by a provider. It should be noted that quality can have a different meaning for different stakeholders. Therefore quality should be evaluated from the perspectives of students, staff and employers. The program's quality should be controlled. Mishra [5] described several aspects of quality assurance for higher education in a book.
The quality of programs is usually evaluated by national accreditation committees. However, only in some countries the national framework for quality assurance takes the level of international higher education into account when evaluating programs. This may affect the status of an institution negatively. In the United States, private educational associations-recognized by the United States government-determine and regulate the educational standards of American universities. The Commission on Accreditation for Health Informatics and Information Management Education (CAHIIM) is such an accrediting organization whose mission is to serve the public interest by establishing and enforcing quality Accreditation Standards for Health Informatics and Health Information Management educational programs. Initially they focussed on accrediting Health Information Management programs but in 2010 they also defined accreditation standards for health informatics master programs [6]. There are now discussions going on between the American Medical Informatics Association (AMIA) and CAHIIM about AMIA's participation in accrediting health informatics master degree programs.
Educational institutions compete for students. The international status of an institution and its programs is important for students. Therefore institutions may invite international experts to evaluate their programs in order to establish a positive international status. This can become a costly business since usually not only the travel and accommodation costs for the experts have to be paid but also they have to be remunerated. If more institutions are interested in an international evaluation of their health informatics programs, IMIA can serve as accreditation agency. The accreditation process can be less costly when experts from member countries of IMIA agree to carry out the peer review for free (expecting only remuneration of travelling expenses and accommodation). To the knowledge of the authors there are no other existing accreditation agencies focussing on health informatics higher education than the IMIA international accreditation and the national accreditation by CAHIIM and AMIA.
On the basis of the assumption that more institutions are interested in an assessment of their programs at an international level, a proposal to start with IMIA accreditation was submitted to the IMIA Board. An accreditation procedure was presented in the proposal. In 2011, the IMIA General Assembly accepted a proposal to test out the accreditation procedure in a trial phase in which about five institutions, spread over the IMIA regions, would volunteer to participate. The IMIA accreditation is an addition to national accreditation and does not replace it.
In this contribution we first explain the general pattern of how accreditation is carried out in various countries. Then we focus on the accreditation procedure developed for IMIA.
II. How Accreditation Is Carried Out
Quality review can be carried out by an institution itself or via an external quality assurance agency. But also in the latter case quality assurance should be a continuous and ongoing process in educational institutions. It should not be a one time activity dedicated to the external review. The advantage of external quality review is that it assures external stakeholders such as employers, professional bodies, students and the general public of the quality of an educational program or educational institution. Quality review can focus on programs but also on institutions. In the latter case the focus is on the way the institution has organized the internal quality assurance system.
There are several approaches to external quality review: accreditation, assessment, and audit. Accreditation determines whether the program meets a certain minimum standard. All aspects of a program such as whether the curriculum is an adequate realization of the intended end qualifications, the quality and quantity of the staff, available facilities, study load, student satisfaction, the student drop-out rate, and the average time of study are assessed. Usually accreditation is either conferred or denied. Whereas accreditation evaluates the quality against a minimum standard, assessment evaluates the output of an institution or program, resulting in a more graded judgment of the quality of a program. Audit focuses on the quality procedures adopted by an institution and not so much directly on the quality of teaching and learning.
The accreditation procedures of different countries show a lot of commonalities. These commonalities are presented here. Before starting accreditation the quality assurance agency must indicate which topics will be assessed and which criteria will be used. These topics and corresponding criteria are laid down in a document. Every institution therefore knows what aspects of the program will be reviewed and how they are evaluated. On the basis of this information the institution prepares a self assessment report. A peer review team validates the report. The peer reviewers usually are experts in the field that is covered by the program. They are invited by the quality assurance agency or are employees of this agency.
The self-assessment report provides the basic information needed by the peer review team to evaluate the assessment criteria. The peer review usually comprises a site visit that may take from one to four days. During the site visit the peer review team (called site visit committee in the IMIA accreditation documentation) consults with the various stakeholders, ranging from the rector and dean to staff, student and alumni representatives, to employers of the graduates of the reviewed programme or institution. The site visit committee may during the site visit ask for more information when needed.
After the site visit the committee prepares a report containing an evaluation of the program (using the earlier mentioned topics and corresponding criteria) and the final judgment. The judgment concerning each facet has to be motivated and references have to be made to the self-assessment report. The institution or program can correct factual errors if they are present in the report. Then the quality assurance agency will make the final decision concerning accreditation.
III. Accreditation Procedure of IMIA
In the proposal for initiating IMIA accreditation a number of decisions with respect to the accreditation procedure were laid down. In the first place it was decided to define quality as fitness for purpose. Since the programs to be accredited can focus on different topics at various levels and can have different orientations (academic programs, vocational programs, PhD programs), the quality of such diverse programs can only be adequately assessed by comparing the described goals of the program (purpose) with how these goals are implemented in the curriculum (fitness for purpose). Of course also the goals themselves should be assessed: is there a need for graduates with the qualifications expressed in the goals?
A second decision was to go for accreditation. This means that a review team will check whether the program meets a certain minimum international standard. This minimum standard can be partly derived from the IMIA Recommendations on Education in Biomedical and Health Informatics.
A third decision made was that the program's reviewers should be peers: experts having experience in Biomedical and Health Informatics education and research.
The accreditation procedure used in the Netherlands and Belgium for academic programs was taken as a template for designing the IMIA accreditation procedure. Institutions interested in accreditation have to write a self-assessment report that in addition to a site visit will provide the members of the site visit committee enough information to assess the program. In the self-assessment report an answer should be given to the following six main questions. In the first place it is asked what the goals of the program are for which the institute asks accreditation and how the goals are implemented in a curriculum. The next questions focus on the resources: what is the size and quality of the staff and which facilities for teaching are available? A fifth question is about quality assurance: how does the institute guarantee the quality of the program? The last question asks about results: are the goals routinely reached?
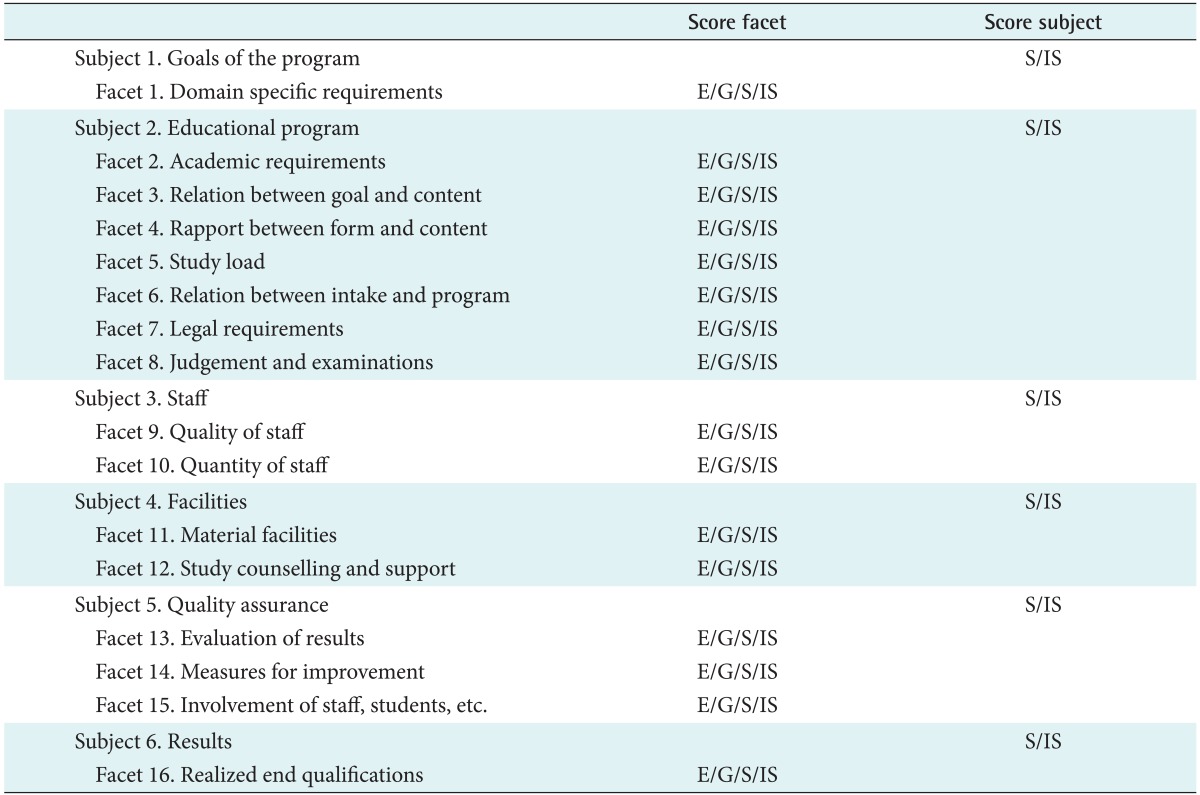
Each of the above six questions concerns a specific subject: goals of the program, contents of the educational program, staff, facilities, quality assurance, and results. The subjects are subdivided in a varying number of so-called facets. In total 16 facets are distinguished. The members of the site visit committee receive a checklist starting with a summary page for copying the judgements of the facets and subjects that the members record in the following pages (Table 1). The checklist is filled in by each reviewer independently during the visit. In Table 1, the names of the subjects and their facets are presented. In the third column the score of each facet is entered (E means Excellent, G means Good, S Sufficient, and IS Insufficient). The last column contains the score of each subject (S is Sufficient and IS Insufficient). There is also an explanation what these scores mean (not shown in the table). Excellent for example means: "best practice", can serve as an example for other programs.
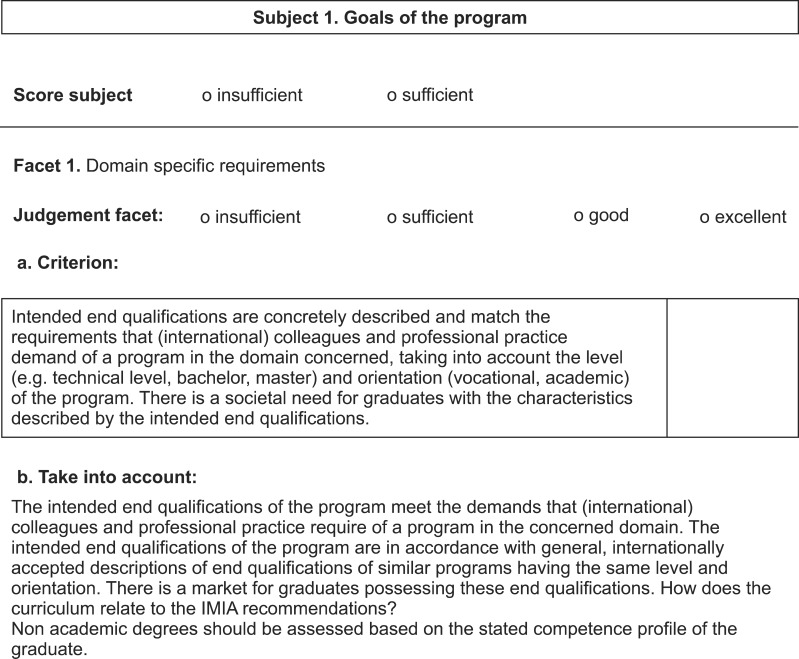
For each facet a criterion is specified. It is also indicated which topics the reviewers have to take into account when assessing that facet (Figure 1). Figure 1 shows the first part of the checklist located after the summary page. In Figure 1, the name of the first (and only) facet (domain specific requirements) of the first subject (goals of the program) is shown. There is space for specifying the judgement of the facet and the score of the first subject (since the first subject only has one facet), the judgement of the first subject is easily deduced from the judgment of the facet. For a full discussion of the subjects and facets the reader is referred to Mantas [7].
Each subject is given the score sufficient or insufficient, based on a weighted judgement of the related facets. Subsequently the quality of the entire program is determined: the quality is positive if all subjects are judged sufficient, else the quality is negative. Only positively evaluated programs will be conferred IMIA accreditation.
1. The Self-assessment Report
To ease the work of the site visit committee, the program management delivers a document (called the self-assessment report), containing a critical reflection about the program. The six subjects mentioned above should be described in sufficient detail so that it is possible for the site visit committee members to evaluate the 16 facets of the accreditation review framework. Both strong and weak points should be described. The report should present the program in such a way that teachers and students recognize and agree with its content. The critical reflection is pre-eminently a means to let teachers, students and the members of the site visit committee discuss the quality of the program.
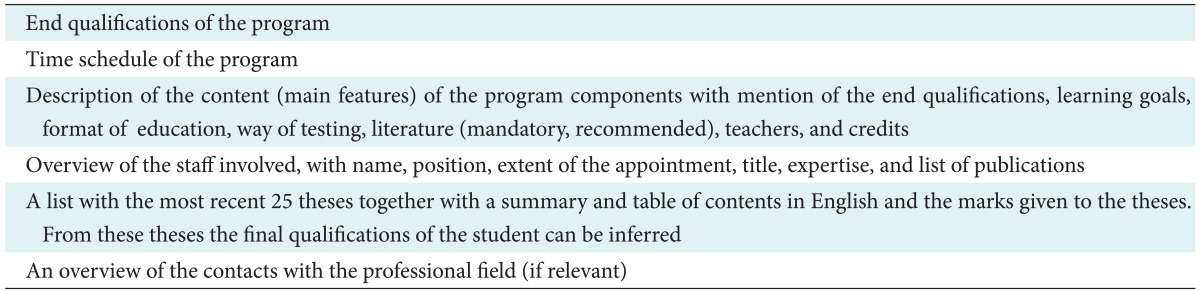
Supporting evidence (like books and other study material) has to be available during the site visit for possible inspection. The program has to provide-in addition to the self-assessment report-a limited number of additional documents. It is assumed that the information for these documents is readily available within the program. The documents serve to substantiate and are possibly used for verification. Table 2 presents the needed documents.
How the self-assessment report should be structured, which additional documents should be added to the self-assessment report and which documents should be available at the site is mentioned in the IMIA accreditation procedure document that is sent to the institution that asks for accreditation. In this report also the review framework is described. This information is also available on IMIA's Website [8]. The framework offers the possibility not only to discuss the results of the past but also the ambitions for the future. What are the choices for the future, in which direction will the program develop? The plans for the future therefore should also be mentioned at the end of the document.
2. Site Visit Process
An institution that wants a health informatics program to be evaluated has to contact IMIA. The chairman of the Accreditation Committee (during the trial period this committee only consisted of the Vice-President (VP) Special Affairs) receives the request and sends the IMIA accreditation procedure document to the institution. As explained above this document contains all information needed by the institution to start the process. The requested documents have to be in the possession of the chairman of the Accreditation Committee one and a half month before the site visit takes place. After sending the IMIA accreditation procedure document the chairman contacts the institution.
It has to be decided which experts will become member of the site visit committee. These members can be suggested by the institution or by the Accreditation Committee chairman. In both cases the other party has to agree about the composition of the site visit committee. The members should not have ties with the institution.
The committee consists of three senior members and the committee as a whole should have at its disposal expertise with respect to the scientific developments in the field of study, international expertise, expertise with teaching and with the development of education at the level concerned, familiarity with the way the education is delivered (distance education, workplace related education, flexible education, traditional education, etc.) and audit expertise.
The Accreditation Committee nominates the chairman of the site visit committee. This person should have experience with leading a site visit committee. Finally the chairman of the Accreditation Committee and the institution settle a date for the site visit.
The chairman of the site visit committee writes a concept Accreditation report after the site visit. The report contains the motivated judgements about the subjects of the review framework. In the report the judgements are corroborated by references to the self-assessment report, the discussions with the representatives of the program and data from the material that could be inspected during the site visit. Possible actions for improvement are presented in a separate section of the report. In addition the report contains the scores of the judgements of the subjects and criteria, information about the date of the site visit, the names of the discussion partners, basic data about the program, and an overview of the studied material. The report is sent to the Accreditation Committee of IMIA after all site visit committee members have agreed with the content.
3. Decision by Accreditation Committee
The Accreditation Committee receives the report from the site visit committee within six weeks after the site visit. The Accreditation Committee will check whether in the report all subjects have been covered, discussed and assessed and then will send the report to the requesting institution within two weeks after the receipt of the report from the site visit committee. The institution can suggest corrections in case of factual errors and provide relevant additional information within a period of two weeks. After the corrections have been made by the site visit committee, the Accreditation Committee decides whether the program will be accredited.
The institution is informed about the decision. If the judgment is positive the program can use the label 'Accredited by the International Medical Informatics Association'. The accreditation status lasts for five years. Then reaccreditation is necessary.
The institution can appeal against a negative decision. The institution can apply again for accreditation after they have corrected identified shortcomings. Depending on the circumstances a new site visit will be necessary.
IV. Testing out the Accreditation Procedure
Since the IMIA accreditation procedure was derived using a framework that was only used in the Netherlands and Belgium it was considered wise to test the procedure on programs established in various countries spread over the globe. Only in this way it can be checked whether the procedure works well for programs of different levels and orientations and in different cultural environments. In 2012 three programs were evaluated and accredited:
1) The Health and Human Services Informatics Master's degree program, University of Eastern Finland, Kuopio, Finland
2) The Biomedical Informatics Technologist Educational Program, DuocUC School of Health, Santiago, Chile (non-academic, vocational, technical level)
3) The Health Informatics Bachelor's degree program and the Health Informatics Master's degree program, Georg-August-Universität, Göttingen, Germany
In 2013 another three programs will be assessed. Other programs have indicated their interest.
The accreditation procedure generally appeared to be adequate. An assessment of the IMIA educational accreditation process is reported elsewhere [7]. Only a few changes had to be made in the procedure. We mention an example of a change in the documentation that was necessary for theses written in the national language. To demand that the program should translate the theses into English was not considered a good idea: it is too time consuming or costly for the program. Instead the program was asked to provide thesis summaries in English.
However, it appeared that the thesis summaries not always provided enough information to get a sufficient impression of the quality and content of the theses when reading them before the site visit. It was decided that in the future a translation of the Table of Contents should also be provided. Of course individual theses (examples of the ones with the highest and the lowest marks) were extensively discussed with the faculty who translated relevant pieces of the theses on the spot.
Another example is an organizational change. During the trial period the VP Special Affairs (A.H.) designed the accreditation protocol and was chairman of the site visit committees. During the last General Assembly of IMIA it was decided to establish an Accreditation Committee within the Board of IMIA (as already described in the accreditation protocol). This committee among others will appoint the members of the site visit committee and the site visit committee will report to this Committee. Until now the VP Special Affairs appointed the committee members. Also all administrative contacts of the institution with IMIA and vice versa are via the Accreditation Committee.
In an earlier article [9] we presented the impressions of the Health and Human Services Informatics program. This two-year master's degree program at the University of Eastern Finland was the first program that was accredited. Their objectives for being accredited were among others to provide to their students and alumni knowledge about their status among health informatics programs internationally, in case they were willing to continue their studies abroad. Also, it was their wish to make the program more visible locally, nationally and internationally. According to the program the self-assessment report model was very well structured and the instructions in the accreditation protocol were clear. They stated that it was very rewarding to analyze the statistics although they noticed that the university's administrative information systems were not producing data they needed and they had to create new manual files as well. It is our impression that also the other two institutions that were accredited were positive about the procedure.
During the trial period until now IMIA has already accumulated substantial experience regarding the process and ways of improving it. The different levels and orientations of the programs, the variety of cultures encountered, and the differences in implementation and infrastructural possibilities provided enough material for us to generalize and refine the accreditation procedure to facilitate its routine use in the future. The common characteristics of all visits, for which we were grateful, were the willingness of the volunteering institutions to assume the costs and time commitment for accreditation, the overwhelming preparation and enthusiasm to participate shown at all levels of their hierarchy, and the acceptance of the final judgment of the committee, which included a number of recommendations.
An Accreditation Review Committee consisting of three independent IMIA Board members evaluated the first three accreditation reports. The committee came to the conclusion that the site visit committees have carefully studied the respective programs, that they documented their reviews and recommendations extensively and well-written in their reports, and that the IMIA Accreditation Review Committee fully supported all three recommendations. In addition it was stressed that in case of reaccreditation the actions for improvement, as expressed in the accreditation report, should have been put into practice. Otherwise reaccreditation is probably not possible.
V. Conclusion
IMIA accreditation can be useful for institutions to show to potential students, be they national or international, that their program in health informatics is of an international level. It can enhance the competitive position of the institution. This was indeed confirmed by the management of the first accredited program. The accreditation protocol, based on the framework used in the Netherlands and Belgium, proved to be usable also in other countries. The protocol appeared to be clearly written so that it was clear for the management of the programs how to write the self-assessment report. The first three site visits were carried out in 2012 and another three will be carried out in 2013. The programs all volunteered. The first three accreditation reports were evaluated by an independent committee of the IMIA Board. Their judgment was positive. The accreditation procedure in general worked well and only a few changes had to be made. To our knowledge IMIA is the only accreditation agency for health informatics programs in the world. As stated before, the IMIA accreditation does not replace the national accreditation, it is an addition. In the United States, AMIA is considering cooperating with CAHIIM for accrediting master degree programs in health informatics.
IMIA accreditation will not be useful for all programs and the national accreditation will suffice for them. However, when a program wants to attract the best national students or also wants to attract foreign students, being accredited by an international organization is very important. Students will select a program taking into account the international status of the program. But not only for attracting the best students accreditation is helpful, programs may also volunteer for accreditation because they want to show the management of their faculty or their university that the program has a status comparable to well-known international programs. The IMIA accreditation protocol proved to be easily comprehensible and the self-assessment reports we have obtained until now (five) were in accordance with the specifications mentioned in the protocol. The accreditation framework developed in the Netherlands and Belgium for arbitrary academic programs appears to be transferable to health informatics programs both at the academic and vocational level.