Computer and Internet Interventions for Loneliness and Depression in Older Adults: A Meta-Analysis
Article information
Abstract
Objectives
This study conducted a meta-analysis to examine the effectiveness of computer and Internet training interventions intended to reduce loneliness and depression in older adults.
Methods
Searches were performed to retrieve studies that had been published in peer-reviewed journals from January 2001 to July 2012 and written in English or Korean from PubMed, CINAHL, Scopus, the Cochrane Library, PsycINFO, KoreaMed, KMbase, KISS, MEDLIS, and RISS. We used combinations of the keywords for population, intervention, and psychosocial problems. A meta-analysis was employed to summarize the findings of studies on computer and Internet interventions for older adults. An overall mean weighted effect size for each outcome was calculated, and Q statistics were used to test the heterogeneity of variance in the effect sizes of the selected studies.
Results
As the Q statistics revealed heterogeneity, random effects models were chosen for the meta-analysis. The overall mean weighted effect size for loneliness from five studies was statistically significant for decreased loneliness (Z = 2.085, p = 0.037). However, the overall mean weighted effect size for depression from five studies was not statistically significant (Z = 1.528, p = 0.126).
Conclusions
These results suggest that computer and Internet programs were effective in managing loneliness among older adults. Therefore, further computer-mediated social support should be considered to help manage loneliness in this population.
I. Introduction
As the increase in the older population (i.e., older than 65 years old) is an imperative social matter in South Korea and other nations, psychosocial problems encountered by older adults, such as loneliness, social isolation, and depression, have been reported as major factors that threaten the quality of life in this population [1]. However, the current lack of social services for community-dwelling older adults could lead to various physical and emotional problems among them [2]. For example, loneliness is significantly associated with decreased activities of daily living [3], health problems [4], cognitive impairment [5], and depressive symptoms [6]. Factors contributing to the loneliness of older adults include lack of social support [7], increased age [6], and related psychological factors (e.g., depression) [6].
In addition, depression is a very common health problem among older adults: 1-4% of the general elderly population has major depression, and the annual incidence rate has been reported to be 0-15%. However, after 70-85 years of age, the prevalence and incidence rate of major depression doubles [8]. In South Korea, depression is even more prevalent in older adults, affecting 20-70% of this group [9]. Depression in older adults has been shown to be highly correlated with a lower quality of life [10], increased healthcare costs [10], and mortality rate [11].
The introduction of computer technology, including the Internet, has changed our lives. In this changed social environment, older adults have more opportunities to use computers in their daily lives for communicating, banking, shopping, health maintenance, seeking leisure activities, and so forth [12]. Moreover, they have currently become the fastest-growing group of Internet users [13] and could active users of health information obtained via Internet [14]. Since the mid-1990s, numerous studies have reported computer learning in older adults, and these studies have extended our understanding of computer usage in this age group. As computer and Internet usage among older adults is becoming an important field, it is necessary to understand how older adults use computers and the Internet to manage psychosocial problems they experience, such as loneliness and depression. Various intervention studies have laid the foundation for understanding how computer and Internet use plays an important role in increasing psychosocial well-being, but also have some inconsistent findings.
Moreover, several systematic reviews and critical syntheses have been conducted based on these previous studies [15-18]. However, they dealt with computer and Internet training as only a small part of intervention studies for reducing older adults' social isolation [16] or included descriptive or correlation studies from all age groups, a practice that prevents us from delineating the effects on older adults [17]. Although one systematic review reported that computer or Internet use did not affect psychosocial well-being in older adults [15], it provides no quantitative evidence of the effectiveness of such interventions on their psychosocial problems and more evidence need to be supplemented with more current data. Therefore, the purpose of the present study was to examine the effectiveness of computer and Internet interventions in reducing loneliness and depression among older adults, through a meta-analysis.
II. Methods
1. Search Strategies
Searches were performed to retrieve studies that were published in peer-reviewed journals from January 2001 to July 2012 and written in English; the following databases were used: PubMed, CINAHL, Scopus, the Cochrane Library, and PsycINFO. We used combinations of the key words categorized as follows: for population, we used older, aged, older adult*, ageing population, senior*, senior citizen*, or elder*; for interventions, technology*, pc, computer*, web, Internet, web-based, online, or e-mail; and for outcomes, depression, loneliness, wellbeing, well-being, wellness, psychological, psychosocial, or social isolation. We also used similar keywords to search articles written in Korean in databases such as KoreaMed, KMbase, KISS, MEDLIS, and RISS.
2. Study Selection
The inclusion criteria were using older adults living in either communities or facilities as the target population, an intervention that involved computer or Internet use, and measuring the psychosocial outcomes (i.e., levels of loneliness and depression) of interest. The following kinds of studies were excluded: those focused on a specific disease or symptom, those that had no experimental design or control group, and those that did not measure loneliness or depression.
Of the 2,518 articles initially obtained, 746 were excluded because of duplication, and 1,749 were excluded after title and abstract review. After reviewing the full text of the remaining 23 studies, six studies [19-24] were included in the final meta-analysis (Figure 1). Seventeen studies were excluded because they were non-experimental studies (n = 4), focused on a specific disease or symptom (n = 7), had no control group (n = 1), had no older subjects (n = 1), and did not measure loneliness or depression (n = 4).
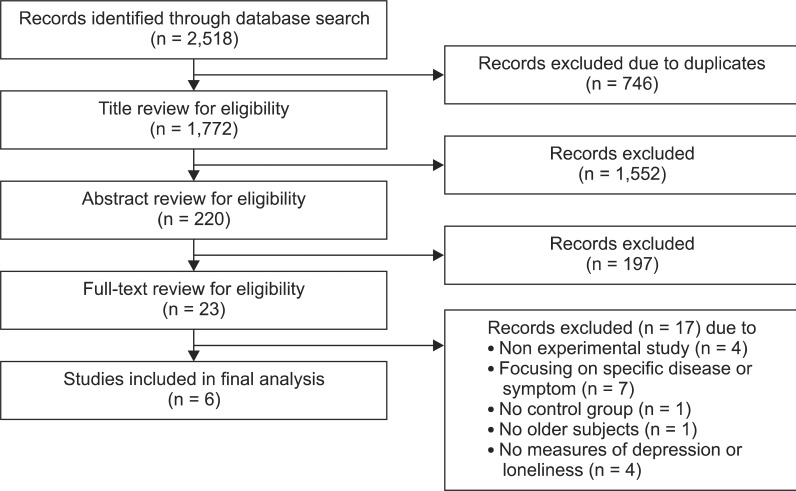
Study selection process.
3. Data Extraction
Data were extracted from the selected articles and put into an electronic data sheet. The contents of the data sheet included year of publication, research question or purpose, study design, sampling methods, study sites (or region), period of study, variables, measurement tools, possible sources of bias, confounding variables, attrition and response rate, analytic methods, effect size and p-values, and 95% confidence interval (CI). In instances of disagreement, each case was discussed by all authors.
4. Statistical Analysis
For calculating effect sizes, Hedges' g formula was used. Hedges' g obtains a standardized effect size by calculating the difference between the mean of the two compared groups divided by the pooled standard deviation. If only a p-value or test statistics (e.g., t or F) were available, those values were converted to g effect sizes. Positive effect sizes represented being in favor of the experimental group. These effect sizes were weighted by study variance. An overall mean weighted effect size for each outcome was calculated as well. To test heterogeneity of variance in the effect sizes of the selected studies, Q statistics were used such that the null hypothesis was that all study treatment effects were equal. When heterogeneity was present, random effects models were considered to provide a conservative estimate (i.e., CI) for the effect sizes.
5. Assessment of Risk of Bias
The Cochrane Collaboration's "Risk of Bias" tool was used to the methodological qualities and risks of bias [25]. It has seven specific areas (sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other bias) from five domains: selection, performance, detection, attrition, and reporting. We employed another tool to assess risk of bias for non-randomized studies [26] for two quasi-experimental studies. Three areas-selection of participants, confounding variables, and intervention measurement-were replaced, as the primary concern of a non-randomized study is limited to guaranteeing similarity between an intervention group and a control group. Each area was evaluated as low risk of bias, high risk of bias, or unclear risk of bias according to the judgment criteria. In instances of disagreement, each case was discussed by all authors.
III. Results
1. General Characteristics of Selected Studies
A total of 373 subjects participated in the six studies. Table 1 shows the summary of participant characteristics of each study included. Out of the six studies, four were randomized controlled trials. The length of intervention ranged from 3 to 36 months, and two studies had a follow-up period of 12 months or more. All interventions included both computer and Internet training, and 4 studies [19,20,22,23] provided computers as well to the older adults they studied. The two psychosocial outcomes of interest in the present study were loneliness (n = 5) and depression (n = 5); four studies measured both.
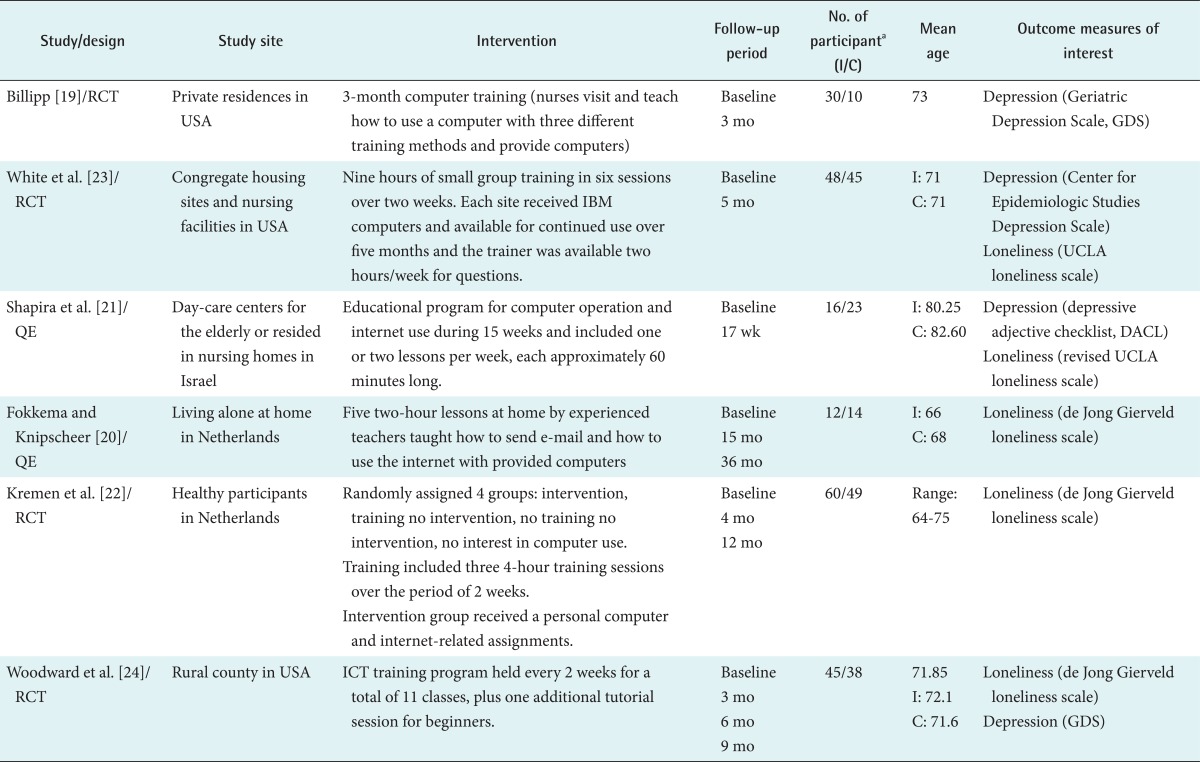
Characteristics of data sources included in meta-analysis of effect of computers use on older adults' loneliness and depression
2. Pooled Results
To test the heterogeneity of variance in the effect sizes of the five studies in each outcome, Q statistics were used. The values of the Q statistics of loneliness and depression were 20.287 (df = 4, p < 0.001) and 30.583 (df = 4, p < 0.001), respectively. Because the Q statistics suggest that those studies were heterogeneous, random effects models were used for the final meta-analysis.
The overall mean weighted effect size for loneliness in the five studies was 0.546 with a 95% CI of 0.033-1.059 (Z = 2.085, p = 0.037) based on data from 353 older adults. Thus, computer and Internet training interventions had effect in decreasing loneliness in older adults. The overall mean weighted effect size for depression in five studies was 0.500 (95% CI, -0.141 to 1.142) based on 344 older adults, which was not statistically significant. Figure 2 shows a forest plot of the mean weighted effect sizes and 95% CIs for both loneliness and depression.
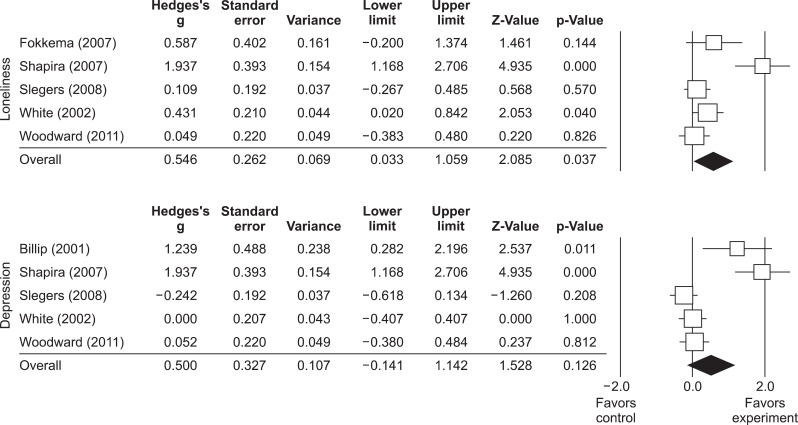
Forest plot for effect sizes and 95% confidence intervals for studies included (random effects model).
3. Methodological Quality and Risk of Bias
Table 2 shows the quality summary and judgments from the risk of bias assessment. Randomization was mentioned in all four randomized studies [19,22-24] but none described the generation of random sequence, allocation concealment, or the blinding of participants and personnel (high or unclear risk). Almost all of the studies (83%) [19,21-24] failed to mention missing or incomplete data explicitly (unclear risk), and one study [20] in particular had a high risk of attrition bias due to the high attrition rate of its subjects, which might have been the result of the long term follow-up period (3 years) for the aged population. None of the six studies indicated whether the methods included the blinding of the outcome assessment, whereas all six studies had low reporting bias. Because of the small number of studies, funnel plot analyses could not determine publication bias.

Summary of risk of bias of selected studies
IV. Discussion
This study was conducted to determine the effectiveness of computer and Internet interventions in decreasing loneliness and depression among older adults. We found that these interventions were significantly effective in decreasing loneliness, but ineffective in decreasing depression. Previous studies reported that older adults were more likely to use the computer and Internet for communication to strengthen existing social networks with family and friends and to develop new social activities that help reduce social isolation, loneliness, and depression, as well as to enhance social support, especially in the presence of mobility and activity limitations [27,28]. However, some researchers suggested that Internet usage has negative or no effects on psychosocial wellbeing [15].
Computer and Internet interventions were effective in decreasing loneliness among older adults in the current study. In other words, a possible reason for these results is that computer and Internet usage are now serving as social supports among older adults, thereby ultimately decreasing their loneliness. Specifically, the results suggested that computer and Internet usage helps older adults to communicate with family and friends as well as obtain news and other useful information [29]. Computer-mediating social support was increased when older adults spent more time using the Internet, had more knowledge of the Internet, were of a lower age group, were women, and had fewer physical barriers [29]. Therefore, when researchers apply computer-mediating social support to older adults, such factors should be considered to help them manage psychosocial wellbeing.
The ineffectiveness of computer and Internet usage on depression among older adults in this study may result from the characteristics of the studies we included. First, two studies had small sample sizes [19,21], which might have limited the generalizability of their results statistically. In general, computer intervention studies tend to have small sample sizes because this kind of intervention needs resources such as computer equipment and spaces. However, one study used a survey design [28] with a large sample size (n = 7,839) and found that computer and Internet use significantly reduced depression in approximately 26% of the participants. Second, the scores on the instruments measuring depression (e.g., Center for Epidemiologic Studies Depression Scale [CES-D] and Geriatric Depression Scale [GDS]) were low at baseline, which indicated that study participants seemed to have low levels of depression. Thus, there was little room for improvement after the intervention. In general, studies on depression require the examination of confounding factors such as age, gender, living arrangement, economic status, education level, cognitive status, activities of daily living, and presence of disease [30]. These factors might influence the effectiveness of computer and Internet interventions for depression. Therefore, in further studies on Internet-based depression intervention, such confounding factors should be controlled for or at least considered.
However, the small number of studies in our meta-analysis limits the generalizability of our own results. In addition, the small number of studies prevents the use of funnel plots to detect publication bias. Further studies should therefore be conducted in this field. However, despite this limitation, our study contributes to existing knowledge in determining the effect of computer and Internet interventions on psychosocial problems among older adults.
In conclusion, computer and Internet interventions were effective in decreasing loneliness, but not depression. Currently, many older adults have the opportunity to use various devices besides a personal computer, such as tablet PCs or smart-devices. In the near future, these devices may play a key role in providing older adults with social networks so that they stay connected with the wider world and obtain new information that has a beneficial effect on their psychosocial wellbeing. Thus, web pages and applications for tablet PCs and smart-devices that older adults find more usable should be developed. In further studies, the effectiveness of these newly developed devices on psychosocial problems should be investigated.
Notes
No potential conflict of interest relevant to this article was reported.