Impact of the Lightwave Health Information Management Software on the Dimensions of Quality of Healthcare Data
Article information

Abstract
Objectives
The use of technology in healthcare to manage patient records, guide diagnosis, and make referrals is termed electronic healthcare. An electronic health record system called Lightwave Health Information Management System (LHIMS) was implemented in 2018 at Cape Coast Teaching Hospital (CCTH). This study evaluated the impact of LHIMS on the quality of healthcare data at CCTH, focusing on the extent to which its use has enhanced the main dimensions of data quality.
Methods
Structured questionnaires were administered to doctors at CCTH to enquire about their opinions about the present state of LHIMS as measured against the parameters of interest in this study, mainly the dimensions of quality healthcare data and the specific issues plaguing the system as reported by respondents.
Results
Most doctors found LHIMS convenient to use, mainly because it made access to patient records easier and had to some extent improved the dimensions of quality healthcare data, except for comprehensiveness, at CCTH. Major challenges that impeded the smooth running of the system were erratic power supply, inadequate logistics and technological drive, and poor internet connectivity.
Conclusions
LHIMS must be upgraded to include more decision support systems and additional add-ons such as patients’ radiological reports, and laboratory results must be readily available on LHIMS to make patient health data more comprehensive.
I. Introduction
In recent times, information technology has emerged as a driving force behind significant advancements across numerous critical sectors, including the health industry. Many developed countries have achieved a prestigious status by investing heavily in technology. The application of technology in healthcare for managing patient records, guiding diagnoses, and facilitating referrals is known as electronic healthcare (eHealth) [1].
Lightwave Health Information Management System (LHIMS) is a health information management software designed for healthcare providers in Ghana [2]. LHIMS serves as an electronic health record system utilised for patient management across all teaching hospitals in Ghana, as well as in facilities operated by the Ghana Health Service. The software stores patients’ data, facilitating rapid access to and retrieval of patient records. By enhancing the data collection process, LHIMS has the potential to ensure the quality of health data collected, stored, and transmitted, thereby supporting the provision of healthcare.
A health management information system is one of the six essential components of a healthcare system, integrating data collection, processing, reporting, and use [3]. Any newly implemented health information system must fulfil health data quality standards. Healthcare data should be accessible, secure, comprehensive, reliable, accurate, up-to-date, and maintainable. The concept of healthcare quality encompasses various facets of patient care [4]. High-quality healthcare is characterised by being effective, efficient, safe, timely, patient-centred, and equitable. A primary way that health systems, such as LHIMS, can enhance healthcare delivery is by improving the quality of healthcare data [5].
The lack of data quality frequently arises from a complex and multifaceted set of reasons. Challenges encountered in software development and adoption, including problems with software design, insufficient documentation, inadequate user training, or delays in system updates, can adversely affect data quality [6]. Software systems that are actively employed in real-world settings are under continuous pressure to adapt to changing requirements, such as new regulations, healthcare workflows, policies, and laws. However, as software evolves, meeting these changing requirements becomes increasingly difficult and expensive, owing to the typical growth in software size and complexity [6].
Improvements and fixes to software are often executed with limited budgets, which can lead to a failure to ensure the high quality of the software, provide adequate training, update documentation, or guarantee accurate data reception and validation. Moreover, it is essential to ensure that various data operations, such as import, export, migration, and transportation, do not inadvertently alter the data. The challenges outlined above are often exacerbated by the disconnect between data creators and data users. In such cases, data users may encounter issues with data quality and bear the brunt of the consequences, while the data creators may not share the same level of concern, interest, or motivation to rectify these issues [7].
This study aimed to determine the impact of using LHIMS on the improvement of healthcare data quality since its implementation at Cape Coast Teaching Hospital (CCTH). The study evaluates the efficacy of LHIMS by examining, from the perspective of doctors, the extent to which it has enhanced various dimensions of healthcare data quality, specifically: timeliness, comprehensiveness, accuracy, consistency, reliability, maintainability, and security.
II. Methods
This study employed a non-experimental, cross-sectional design. The research was conducted with doctors at the CCTH in the Central Region of Ghana. CCTH is a tertiary care facility with a bed capacity of 400 and functions as the primary referral centre for both the Central and Western regions of Ghana.
A random sampling method was employed to select 55 participants for the study. The primary tool for data collection was a structured questionnaire, which included both closed and open-ended questions. Data collection occurred from the first week of March 2022 to the last week of June 2022. For data coding, entry, and analysis, we utilised SPSS version 21 and Microsoft Excel 2013. We measured the dimensions of health data quality using Likert-scale indicators, which ranged from “strongly agree” to “strongly disagree.”
The Ethical Clearance Committee of CCTH approved the study to be conducted in the facility. Respondents were given a comprehensive explanation of what the study entailed, and their participation was voluntary and not under any form of duress.
III. Results
Table 1 presents the sex distribution of the respondents, with males constituting 60% and females 40%. The table also details the duration of employment at CCTH: 40% of respondents had been working there for 1–5 years, around 35% for less than a year, and 26% for more than 5 years at the time of the research. House officers comprised approximately 44% of the interviewed respondents, making them the largest group. Residents accounted for only 16%, while consultants represented about 13%. Specialists and senior specialists were the least represented, with 9% and 7% of respondents, respectively, holding these positions at CCTH when the study was conducted.

Sex distribution, ages, and active working period of respondents
Table 2 shows that a majority of respondents acknowledged that the use of the LHIMS has enhanced the timeliness of patient records. About 51% agreed with this statement, 35% strongly agreed, and only 15% disagreed. The table also illustrates that a substantial majority confirmed that the LHIMS has improved access to patient records. Around 60% concurred with this claim, with 36% expressing strong agreement and a mere 2% strongly disagreeing. Furthermore, a modest majority of respondents recognised that the implementation of the LHIMS at CCTH has increased the accuracy of patient health records. This group comprised 30 respondents, with 42% agreeing and 13% strongly agreeing. In contrast, a significant number of respondents (n = 25) held opposing views, with approximately 44% disagreeing and 2% strongly disagreeing with this assertion.

Impact of the usage of LHIMS on the various dimensions of quality healthcare data (timeliness, accessibility, and accuracy)
Table 3 indicates that a majority of respondents (n = 29), representing 53%, disagreed with the claim that the LHIMS had enhanced the comprehensiveness of patient records at CCTH. Conversely, about 33% of respondents agreed with this statement, and 15% strongly agreed. Regarding the currency of patient records, most respondents believed that the LHIMS had improved the timeliness of patients’ health data, with 62% agreeing and roughly 26% strongly agreeing. Only a minority, 13%, disagreed with this view. Furthermore, approximately 73% of respondents agreed, and 18% strongly agreed, that the LHIMS had increased the consistency of patient health data at CCTH. In contrast, about 9% of respondents did not agree with this statement.
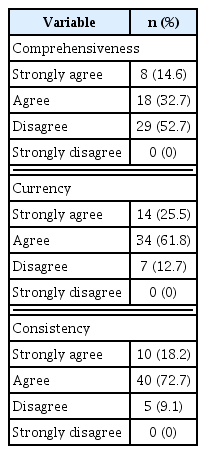
Impact of the usage of LHIMS on the various dimensions of quality healthcare data (comprehensiveness, currency, and consistency)
Table 4 shows that the majority of respondents (54 in total) believe that utilising the LHIMS at CCTH can be challenging at times. Within this group, about 62% strongly agreed with the statement, 36% agreed, and a single respondent, accounting for 1% of the sample, disagreed. The table illustrates the challenges encountered by respondents when using the LHIMS. An unstable internet network was identified by approximately 58% of respondents as a significant issue, followed closely by inadequate logistics and erratic power supply, each cited by 55% of respondents as common challenges. A smaller proportion of respondents, approximately 6% and 7% respectively, pointed to the unwillingness of health workers to adapt to change and the inadequate training of health workers as additional obstacles.

Challenges encountered by doctors using LHIMS at CCTH
IV. Discussion
The implementation of LHIMS has markedly improved the timeliness of patient records at CCTH. This improvement aligns with findings from prior studies investigating the advantages of eHealth systems, including LHIMS [8]. According to the registries of patient outcomes released in 2019, eHealth systems have been shown to increase the accessibility of electronic health data, thereby enriching real-world data [8].
Accessibility, as a dimension of quality healthcare data, refers to the ease with which patients’ data can be obtained and legally accessed, with robust protections and controls integrated into the process [9]. In this study, 96% of participants confirmed that the LHIMS improved the accessibility of patient records or data. This supports the widely recognised notion that the adoption of eHealth systems can significantly enhance access to patient records. Observations of LHIMS usage at CCTH revealed that doctors are assigned unique usernames and passwords to access the system. Consequently, patient records are safeguarded against access by other individuals or healthcare workers who are not directly involved in the patient’s care. For the doctors, access to the patient’s records is straightforward, and LHIMS cannot be accessed by anyone without the permission of the doctors directly responsible for the patient’s management. These findings align with the study by Black et al. [10], which assessed the benefits of eHealth systems and demonstrated that such systems substantially improve the accessibility of healthcare data.
Patients’ health records are considered comprehensive when they include all necessary data items to be understandable [11]. Among the respondents, 53% disagreed with this statement, 33% agreed, and 15% strongly agreed. Currently, the state of LHIMS at CCTH falls short in terms of integrating all components of patients’ health data. Upon examination of the LHIMS by the investigator and doctors with firsthand experience, it was discovered that key elements such as radiological and histopathological reports, seizure charts, and input and output charts have not yet been integrated into the system. Consequently, doctors must depend on paper or hard copies of radiological reports, including plain radiographs, computed tomography scans, ultrasounds, and so on. The study by Sutton et al. [12] also recommended incorporating radiological and histopathological reports into clinical decision support systems to ensure a comprehensive electronic health record. Furthermore, a study by Hsu et al. [13], conducted in 2012 on context-based electronic medical records, found that a concise presentation integrating relevant information from various sources can enhance the efficiency and comprehensiveness of patient medical records, thereby improving medical decision-making [13].
Accuracy is a critical aspect of high-quality health data, indicating the degree to which the data are devoid of identifiable errors [14]. Most respondents confirmed that the implementation of the LHIMS at CCTH has enhanced the accuracy of patient health records. Of these respondents, around 42% agreed and 13% strongly agreed with this statement. Conversely, a minority of respondents, constituting 44%, disagreed with this assessment.
This outcome is anticipated, as one of the many advantages eHealth systems bring to healthcare delivery is the substantial reduction in errors, which is a key aspect of their design. The information entered by doctors is more readable, and incorrect spellings of medical terms and medications can be easily corrected. This ensures a seamless continuity of care, with patient records being clear to all healthcare workers, especially doctors and nurses who are responsible for implementing treatment plans established by their superiors. The paper record system did not allow for this level of clarity; the legibility of patient records was highly variable and depended on the handwriting of doctors, who often sacrificed legibility for speed in order to see the many patients waiting at the outpatient department. Keasberry et al. [15] demonstrated in their research that electronic health record functions lead to improved organisational efficiency, greater accuracy of information, and reduced documentation and process turnaround times. However, a minority dissented, citing that LHIMS still had significant room for improvement in terms of decision support systems. Ultimately, the responsibility for patient treatment decisions rests predominantly with the doctors, and there remains a risk of diagnostic and treatment errors if doctors do not exercise due caution. The current state of eHealth systems in developing countries like Ghana falls short of expectations when compared to those in developed nations. A study by Zayyad and Toycan [16] in 2017 in Nigeria highlighted that in developing countries such as Nigeria, the adoption rate of eHealth is either low or the systems are underutilised, often lacking critical features like decision support systems.
The concept of the currency of patients’ health data pertains to how current and up-to-date the information is [9]. A substantial majority of survey participants believe that the implementation of Local Health Information Management Systems has improved the timeliness of patient records. About 62% of respondents agreed, while an additional 26% strongly agreed with this statement. In contrast, a mere 13% disagreed. This is likely because LHIMS greatly facilitates the ease of accessing and updating patient records. The system allows for simple access and modification of patient records at any time, enabling doctors to easily consult historical notes. Zhang et al. [17] evaluated the advantages of using electronic health records in residential aged care facilities across Australia. The findings confirmed that the adoption of eHealth systems significantly enhances the currency of health data.
The consistency of patient health data refers to patient records being the same across systems and in the same format as prior data [11]. The majority of respondents supported the idea that LHIMS has improved the consistency of patient health data. About 73% of respondents agreed, while 18% strongly agreed with this idea. Zhang’s research [17] suggested that electronic health records systems maintain data consistency both when it is stored and during transfer. Furthermore, users could access all necessary information across all systems at any time [17].
In evaluating the perceived difficulty of using LHIMS, all respondents agreed that the system can indeed be challenging at times. Follow-up interview questions aimed to delve into these specific challenges from the perspective of the doctors who interact with the system first-hand. The reasons provided by respondents encompassed a range of issues, as expressed in their own words, including, but not limited to, the following.
Respondent 1: “LHIMS is sometimes inaccessible to users due to network issues, and it lacks some clinical parameters (such as seizure charts, etc.).”
Respondent 15: “Whenever there is a power outage, LHIMS does not work.”
Respondent 25: “The server goes off when there is a power outage. At certain times, nurses do not see doctors’ reviews although they would have typed them, requesting labs and prescribing medications can be very frustrating as laboratory technologists and pharmacists do not see requests and prescriptions at their end. This makes house officers and patients go back and forth, thus wasting time and energy.”
Respondent 35: “Unstable network, incomplete patient information that is radiological reports and other charts are not included in the LHIMS.”
Respondent 45: “The inadequate computers provided by CCTH coupled with the poor network increases time spent seeing patients as data entry becomes cumbersome.”
In an effort to prioritise these challenges, they were presented as options in a survey for respondents to select those they considered most relevant to the use of LHIMS at CCTH. The findings were as follows: approximately 58% identified unstable internet networks as a primary concern, with 55% of respondents citing inadequate logistics/technological infrastructure and erratic power supply as significant obstacles. Additionally, a small number of respondents pointed to the reluctance of health workers to embrace change and the insufficient training of health workers, accounting for 6% and 7%, respectively, as other factors hindering the use of LHIMS at CCTH. These results align with similar research investigating the difficulties faced during the implementation and operation of eHealth systems in developing countries [18–20]. A study from 2012 highlighted four main challenges to the adoption of information and communication technology (ICT) and the successful deployment of health information projects: unstable electric power supply, poor internet connectivity, resistance to new technology, and a lack of maintenance culture [18]. Furthermore, research by Bedeley and Palvia [21] examining eHealth issues in Ghana identified inadequate technological infrastructure or ICT logistics and poor internet connection as the leading problems affecting the efficient use of eHealth systems in the country. The study indicated that the most prevalent challenges included erratic power supply, insufficient logistics, and unstable internet connectivity. Doctors who regularly use LHIMS at CCTH suggest that addressing or eliminating these issues would significantly improve the system’s effectiveness.
However, despite the issues present, a majority of doctors (71% of respondents) at CCTH still found the LHIMS convenient to use. The study assessed how LHIMS usage at CCTH has impacted various dimensions of quality healthcare, including timeliness, comprehensiveness, security, consistency, currency, reliability, and accuracy. It was found that LHIMS has enhanced most of these quality dimensions, with the notable exception of the comprehensiveness of patient records. This shortfall is attributed to the doctors’ perception that LHIMS fails to encapsulate the full spectrum of patients’ health records. Critical health information such as radiological reports, seizure charts, urine output charts, and additional laboratory results are not integrated into LHIMS. Furthermore, a considerable number of respondents expressed dissatisfaction with the decision support systems within LHIMS. The decision support capabilities of LHIMS lack crucial elements, including drug dosing alerts, patient allergy alerts, drug-drug interaction warnings, and spellcheck functions.
The study’s scope was limited to doctors, which represents a significant limitation. Including other healthcare professionals in the care delivery process could have provided a more comprehensive understanding of experiences with LHIMS, potentially influencing the study’s results.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.