Need for Information and Communication Technology during COVID-19: An Exploratory Study Using Nurses’ Activity Diaries
Article information

Abstract
Objectives
The coronavirus disease 2019 (COVID-19) pandemic has led to high levels of burnout among nurses. Information and communication technology (ICT) may offer a solution to prevent a potential collapse in healthcare. The aim of this study was to identify areas where ICT could provide support, by analyzing the work of nurses during the COVID-19 pandemic.
Methods
This retrospective exploratory descriptive study analyzed qualitative data from the activity diaries of seven nurses working in COVID-19 wards or intensive care units.
Results
The nursing work process during COVID-19 involved “added tasks,” “changed tasks,” and “reduced tasks” compared to the pre-COVID-19 situation. Nurses reported difficulties in communicating with other healthcare professionals both inside and outside the isolation room, as well as with patients. The use of various ICT solutions, such as real-time video-conferencing systems or mobile robots, could enhance patient monitoring in the isolation room and improve the quality and efficiency of communication.
Conclusions
The changes in work tasks not only led to nurse exhaustion but also negatively impacted the quality of care. ICT solutions should be explored to minimize the time spent in the isolation room, thereby reducing the risk of infection spread. This could also enhance communication among patients, family caregivers, and healthcare professionals.
I. Introduction
Coronavirus disease 2019 (COVID-19), a respiratory infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has spread rapidly worldwide since its initial outbreak in Wuhan, China in December 2019. The World Health Organization [1] declared it a pandemic on March 11, 2020, signifying the outbreak as a significant threat to global public health [2]. Amidst this pandemic, nurses, who play a crucial role in combating COVID-19, have experienced an unprecedented level of stress. This stress poses a threat to their physical and psychological health, their well-being, and the quality of care they provide to their patients [3]. As frontline healthcare workers, they dedicate a significant amount of time to providing direct care to affected patients.
The workload and working hours of nurses have significantly increased due to the influx of COVID-19 patients [4]. The implementation of prophylactic measures, such as donning and doffing protective equipment, carrying out specific decontamination procedures, and managing isolation zones, has further added to the nursing workload [5]. In particular, the necessity of wearing a full set of personal protective equipment (PPE) for extended periods induces tension and fatigue, thereby exacerbating the challenges of nursing work [5,6]. With visitation restrictions in place due to the highly contagious nature of COVID-19, nurses have also had to assume the roles typically played by patients’ families [5]. The surge in COVID-19 patients, coupled with a severe shortage of material and human resources, has made it increasingly difficult for nurses to perform their regular duties [7].
Nurses have experienced high levels of burnout during the COVID-19 pandemic. Preliminary reports have identified several factors contributing to this burnout, including an excessive workload, a high risk of infection, emotional exhaustion, and a limited availability of both material and human resources when caring for COVID-19 patients [7,8]. This burnout among nurses directly leads to a high turnover rate and decreased efficiency in their daily work. This could potentially lead to the collapse of a sustainable healthcare system, especially with the prolongation of the COVID-19 pandemic [9]. Additionally, healthcare organizations have struggled to meet staffing demands and have been unable to provide frontline workers with adequate supplies and PPE [10]. Consequently, the COVID-19 situation has had a profound impact on nurses and the quality of nursing. There is a pressing need to explore work processes and nursing routines in order to reduce nurse burnout and improve their work environment [4,7].
It has been reported that information and communication technology (ICT) can aid in nursing and medical tasks [11]. In particular, the COVID-19 pandemic has underscored the role of ICT as a potential solution to prevent a potential medical system collapse due to nurse burnout and decreased work efficiency [12]. With the global spread of COVID-19, numerous studies have investigated the factors affecting nurses’ physical and mental health. However, there is a lack of prior research analyzing nursing work for ICT utilization. It is crucial to understand which types of ICT can assist with the daily incidents that occur in COVID-19 wards.
This study aimed to explore the areas where ICT support is possible through an analysis of nursing work. By examining the tasks involved in caring for COVID-19 patients and identifying the needs of nurses, efficient ICT interventions can be developed. This approach will not only help to lessen the workload of nurses, but also lay the groundwork for a robust healthcare system capable of handling national crises.
II. Methods
1. Research Design and Sample
This retrospective exploratory study analyzed the qualitative data derived from nurses’ activity logs. The research involved seven nurses employed in the COVID-19 ward, intensive care units, and community treatment centers across six medical institutions. Participants were sourced through network recruitment, a strategy selected to ensure a diverse representation of hospitals and wards, including intensive care units, internal medicine wards, and community treatment centers.
2. Measures and Data Collection
A structured activity diary was used to collect data from September 2021 to October 2021 (Appendix 1). This diary format was originally developed by Oddsdottir and Sveinsdottir [13], and we adapted it to suit the specific needs of this study, drawing on the work of Humphreys et al. [14]. Activity diaries can be either structured or unstructured, offering a framework for collecting large amounts of data and recording situations in real time [15]. These diaries and logs have proven useful in capturing the impact and complexity of activities, as well as in examining the work practices of healthcare professionals [14]. Goemaes et al. [16] employed an activity diary, also developed by Oddsdottir and Sveinsdottir [13], to study how advanced practice nurses use their time and to investigate how time usage varies based on factors such as the type of healthcare organization, work experience, and supervisor. Sveinsdottir et al. [17] used this method to document and reflect on the actual work activities of nurse unit managers in surgical and internal medicine services, as described in their job descriptions. This method is particularly useful for understanding changes in work practices, especially in situations where accessing the ward is challenging due to the infectious nature of COVID-19.
In previous studies conducted by Oddsdottir and Sveinsdottir [13] and Humphreys et al. [14], nurses were instructed to document their tasks at 15-minute intervals throughout their shifts. However, the objective of this study was to generate primary data to aid in the development of ICT interventions. These interventions aim to pinpoint and address the inefficient and time-consuming aspects of nursing work during the COVID-19 pandemic. As such, we modified the 15-minute interval recording method to instead document the time each task took to complete, without any time constraints. Instead of providing a pre-coded task list, nurses were asked to write down their tasks directly. This was done to identify any tasks that were added or newly introduced due to COVID-19. To gauge the difficulty level of each task, we utilized a 5-point Likert scale. If a task was deemed particularly challenging, the reason was noted. While there is no universally agreed-upon sample size for this type of study, Humphreys et al. [14] used a sample of six participants, and Oddsdottir and Sveinsdottir [13] included 15 nurses in their research. Following their methodologies, our study also recruited a sample of seven nurses. Each nurse was given an activity diary via email and asked to record their tasks. Detailed records were necessary to identify any suggestions from the nurses or problems that arose during each task. However, due to the difficulty of recording detailed notes while wearing PPE, the nurses completed their activity diaries by recalling their tasks from the previous 7 days.
3. Data Analysis
Three members of the project team independently and collectively reviewed the completed diaries for errors and ambiguities. Any queries or sections that required further investigation were identified and subsequently discussed with the participants through email or phone interviews.
A thematic analysis was conducted using the activity diary, which entailed a systematic evaluation of each entry. Activities were categorized according to their respective work types, and any tasks added due to COVID-19 were identified by creating a new category. A comparative analysis was then performed, focusing on tasks that were reduced, expanded, or altered. For the quantitative aspect of the work difficulty analysis, descriptive statistics were computed using Microsoft Excel version 16.0.
4. Ethical Considerations
This study was conducted in accordance with the World Medical Association’s Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Participants. Also this study was approved by the Institutional Review Board of Gachon University on July 15, 2021 (No. 1044396-202106-HR-125-01).
III. Results
1. High-Frequency Tasks Time Required for Tasks, and Difficulty of Tasks
All the participants in the study were women, with an average employment duration of 7.3 years and an average age of 31.6 years. The most common task was donning and doffing PPE, which on average took 12.1 ± 3.1 minutes and 11.7 ± 5.4 minutes, respectively. The task that required the most time was inpatient and transfer nursing, taking an average of 51.3 ± 35.1 minutes. The task perceived as the most difficult was changing positions, scoring an average difficulty rating of 4.6 ± 0.4 points (Table 1).

Time required and mean difficulty for each task (n = 7)
2. Changes in Tasks during COVID-19
Since the outbreak of COVID-19, numerous new nursing tasks have emerged, while existing tasks have either been reduced or adapted. The new tasks include cleaning and environmental management, patient transfer, preparation for sample transfer, donning and doffing PPE, and organizing and delivering patient parcels. Adapted tasks encompass admission nursing assessment, vital sign checks, communication within and beyond the isolation room, procurement of material resources, allocation of additional human resources, position changes, and obtaining guardian consent for treatment and procedures. Tasks that have been reduced include nurse handovers, physician rounds, nurse rounds, discharge education, family caregiver visits, and explaining patient conditions (Table 2, Figure 1, Appendix 2).

Comparison table of tasks before and during the COVID-19 pandemic
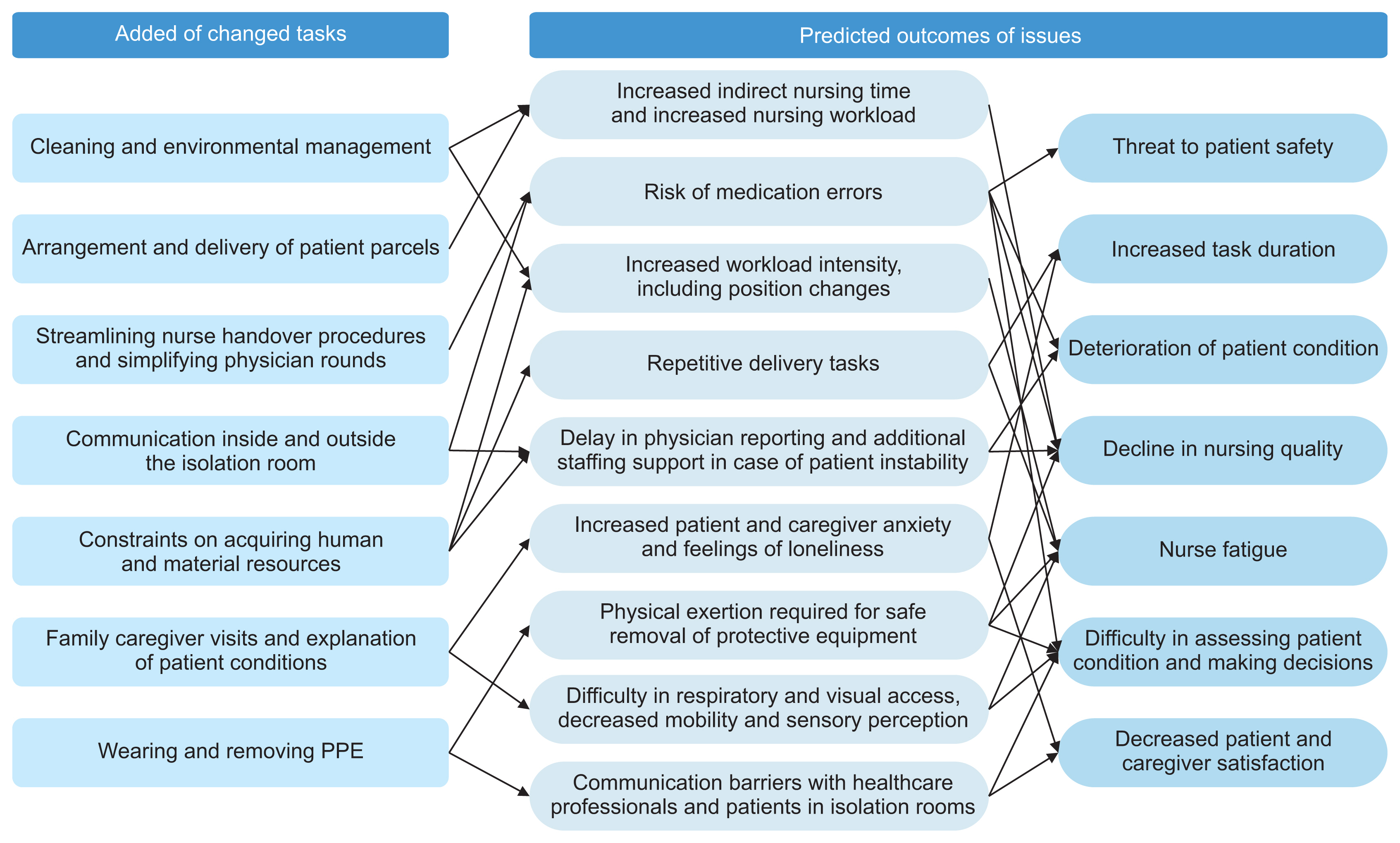
Changes in tasks during the COVID-19 pandemic. PPE: personal protective equipment.
IV. Discussion
Given the ongoing global impact of the COVID-19 pandemic and the critical role nurses play in addressing this public health crisis, this study has highly significant findings. This study illuminated specific areas where ICT support can reduce nurses’ workload and improve their working conditions, thereby contributing to the creation of targeted interventions and bolstering the overall resilience of healthcare systems in times of national crisis. Moreover, the distribution of these research findings and the encouragement of further related studies will promote collaboration and the exchange of knowledge. This will empower healthcare professionals and policymakers to make well-informed decisions and put into action effective strategies to tackle the challenges brought about by the pandemic.
Upon analyzing the activity diaries kept by the nurses, we found that the nursing work process involved “additional tasks,” “changed tasks,” and “reduced tasks” compared to the pre-COVID-19 situation. Among the “additional tasks,” the most frequently occurring task was the donning and removal of PPE.
Regarding PPE, participants reported difficulties with vision and breathing, as well as a sense of impaired mobility. They also noted that it was challenging to promptly and accurately assess a patient’s condition while wearing PPE. The process of donning and removing the protective gear was particularly difficult without assistance from other staff members [18]. The strain of repeatedly putting on and taking off PPE, as well as the fatigue associated with this process, was previously highlighted in a 2015 study on Middle East respiratory syndrome (MERS) [19]. Given that nurses must stay with patients throughout their shifts, they must endure the discomfort of wearing PPE for extended periods [19,20]. This can increase the risk of physical discomfort and pressure ulcers [21]. Furthermore, prolonged hospital stays can increase the risk of infection for healthcare professionals [20], which in turn can heighten nurses’ anxiety levels. The isolation resulting from infection, or the departure of nursing staff due to heavy workloads, can lead to a decrease in available human resources [22]. This could potentially create a vicious cycle, resulting in a decline in the quality of nursing and medical care [23]. The implementation of advanced monitoring systems could help to reduce unnecessary exposure and optimize resource allocation [A7,A10]. For healthcare organizations, it is crucial to promote the adoption of integrated electronic health record systems. These systems facilitate seamless communication and information sharing among healthcare professionals [A11], enabling efficient coordination, timely updates, and collaborative decision-making in the management of COVID-19 cases.
A limited number of people are permitted to enter the isolation room, leading to additional responsibilities such as material transfer, waste disposal, post-patient discharge cleaning, and environmental management tasks. This increase in indirect nursing time escalates the workload, resulting in excessive stress [22]. The preparation for sample transfer has also expanded the nurse’s duties, now encompassing sterilization and wrapping of the container after sample collection, such as a blood sample. Furthermore, with family caregivers prohibited from visiting, nurses have taken on the task of receiving, organizing, and delivering personal items necessary for the patient. This increase in repetitive and non-essential tasks may detract from crucial nursing interventions, such as patient assessment, position changes, oral care, and the opportunity for assessment during these processes [22]. The use of mobile robots for item transfer [A3,A4] or cleaning robots for environmental management can help reduce cross-infection among patients [A1,A2]. Moreover, these technologies can effectively lessen the workload of healthcare professionals [24]. It is crucial to actively seek and test innovative technologies that can efficiently eliminate repetitive and non-essential nursing tasks, thereby promoting increased efficiency and improved workflow. Further research is needed in this area to effectively identify and implement these technological solutions.
The results of this study show that the participants experienced challenges in communicating with healthcare professionals both inside and outside the isolation room, as well as with patients, due to their PPE. The quality of care within medical institutions and community treatment centers is significantly influenced by the communication between patients, nurses, and healthcare professionals [25]. To address these communication issues, the study participants offered insightful suggestions, proposing the potential application of existing commercially available devices such as electronic blackboards and smart glass to improve communication precision. However, it is crucial to acknowledge that there is a current dearth of research exploring the usability and effectiveness of these proposed solutions. As such, additional research is necessary to comprehensively examine the feasibility and potential advantages of implementing these technologies in healthcare environments.
The study participants identified communication inefficiencies not only among healthcare professionals but also during nursing information interviews, explanations of treatment and procedures to family caregivers, and the consent process at admission. These challenges occur when patients cannot be interviewed directly, and the statements of family caregivers become the primary sources of information. Moreover, obtaining consent via phone-based communication can impede the accurate conveyance of crucial details and restrict opportunities for in-depth discussions. The study overall highlights significant difficulties in accurately communicating hospitalization information and procedure consent due to the reliance on phone-based communication methods. Therefore, various commercial ICT solutions or software programs, such as artificial intelligence (AI) speakers, Bluetooth earphones, smartphone applications, and real-time video-conferencing programs used in fields outside of healthcare, could be considered to enhance communication quality and efficiency [26]. Additionally, it has been reported that several hospitals have attempted to use speech-to-text technology to convert voice information into text, thereby preventing information omission and improving record integrity. However, further research is required in this area [27]. Furthermore, the use of voice translation functions could potentially improve communication efficiency with foreign patients.
Given the prohibition on family caregiver visits, it becomes impossible to educate them on discharge procedures. This heightens the likelihood of omitting crucial discharge education, such as post-discharge precautions and outpatient treatment for patients. Consequently, this leads to increased anxiety among family caregivers and a decrease in their satisfaction. Therefore, the transition between inpatient and outpatient settings is a critical factor in improving patient outcomes [28]. In order to address the needs of family caregivers in relation to medical services, and to alleviate their psychological issues such as anxiety and stress caused by hospitalization and visitation restrictions, it is essential to explore the use of video visit systems [A15,A18]. Furthermore, video visits can be particularly effective in a pandemic situation as they reduce direct contact, and they are not constrained by time or location due to their virtual nature. From the perspective of healthcare professionals, video visits provide an opportunity to explain the patient’s condition to caregivers and share a care plan, thereby reducing their workload [29].
It was also reported that essential tasks, which could influence patient treatment and nursing outcomes, have been reduced. Specifically, handovers and rounds conducted by various healthcare professionals are crucial nursing actions for maintaining care continuity [30]. However, due to the constraints of the isolation room, nurses are unable to enter to assess the patient’s overall condition and evaluate the medication and injection site. Patient safety-focused nursing activities include patient education and identification, fall prevention, infection control, and prevention of medication errors [A19]. Consequently, a reduction in these activities could heighten the risk of medication errors and directly jeopardize patient safety. During rounds, only a limited number of individuals are permitted to enter the isolation room. This restriction hampers the sharing of treatment plans due to decreased communication among healthcare professionals. Moreover, in emergency situations, the response of additional personnel may be delayed, increasing the likelihood of the patient’s condition worsening during this delay. Therefore, it is essential to employ “untact” (or “contactless”) technologies such as telepresence systems, CCTV, and mobile robots that can easily monitor the condition of patients in the isolation room and facilitate communication with them [A5].
This study has some limitations. First, the results may diverge from previous studies due to the reliance on participants’ memory when recording their activity diaries. As the analysis was based on the diaries of seven nurses, the generalizability of the findings across diverse medical institutions is limited. Second, despite the potential for variability in hospital policies regarding COVID-19, influenced by factors such as hospital size, environment, and geographical location, our study did not thoroughly evaluate the impact of these variations. Therefore, it is essential to replicate this study with a larger sample of healthcare professionals. Finally, it should be noted that the situation regarding COVID-19 has undergone significant changes since the data collection for this study, which may complicate the interpretation of the results.
The COVID-19 pandemic has led to an increase in non-nursing duties due to a decrease in the number of people allowed in isolation rooms and a shortage of staff. This has made communication between patients, family caregivers, and healthcare professionals challenging. The additional workload has not only exhausted nurses but has also negatively impacted the quality of care. These findings underscore the importance of ICT support in addressing the challenges faced by nurses during the COVID-19 pandemic. By implementing targeted ICT interventions, we can lessen the burden on nurses, improve their work environment, and bolster the resilience of healthcare systems during national crises. Further research is required to confirm the effectiveness of the specific ICT solutions mentioned in this study and to identify innovative technologies that can reduce repetitive tasks for nurses. Healthcare organizations should consider adopting integrated electronic health record systems and exploring technologies such as telepresence systems and mobile robots. These tools can optimize communication and enhance patient safety in isolation rooms.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgments
We would like to thank the nurses who participated in this study.
This work supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2021R1F1A1045487).
References
Appendix
Appendix 1 A structured activity diary used in the study
A Day in the Life of a General Ward Nurse for COVID-19 Patients
< Writing Guidelines >
Please refer to the examples and then delete them before writing.
If there are not enough rows, please add additional rows to complete the writing.
Please record all nursing duties and activities, including nursing practice, breaks, meetings, and documentation, as detailed as possible.
Please write down your recollection of the past 7 days of work.

Appendix 2 List of additional references
A1. The Robot Report Staff. Nimbus robot uses microburst spray to kill coronavirus, other pathogens [Internet]. Santa Barbara (CA): The Robot Report; 2020 [cited at 2023 Jul 22]. Available from: https://www.therobotreport.com/nimbus-robotuses-microburst-spray-kill-coronavirus/.
A2. Begic A. Application of service robots for disinfection in medical institutions. In: Hadzikadic M, Avdakovic S, editors. Advanced Technologies, Systems, and Applications II. Cham, Switzerland: Springer; 2018. p. 1056-65. https://doi.org/10.1007/978-3-319-71321-2_89
A3. Bacik J, Tkac P, Hric L, Alexovic S, Kyslan K, Olexa R, et al. Phollower—the universal autonomous mobile robot for industry and civil environments with COVID-19 germicide addon meeting safety requirements. Appl Sci 2020;10(21):7682. https://doi.org/10.3390/app10217682
A4. Kriegel J, Rissbacher C, Reckwitz L, Tuttle-Weidinger L. The requirements and applications of autonomous mobile robotics (AMR) in hospitals from the perspective of nursing officers. Int J Healthc Manag 2022;15(3):204-10. https://doi.org/10.1080/20479700.2020.1870353
A5. Ma AC, Meng Z, Ding X. Performance review of intelligent guidance robot at the outpatient clinic setting. Cureus 2021;13(8): e16840. https://doi.org/10.7759/cureus.16840
A6. Payne TH, Alonso WD, Markiel JA, Lybarger K, White AA. Using voice to create hospital progress notes: Description of a mobile application and supporting system integrated with a commercial electronic health record. J Biomed Inform 2018;77:91-6. https://doi.org/10.1016/j.jbi.2017.12.004
A7. Barnawi A, Chhikara P, Tekchandani R, Kumar N, Alzahrani B. Artificial intelligence-enabled Internet of Things-based system for COVID-19 screening using aerial thermal imaging. Future Gener Comput Syst 2021;124:119-32. https://doi.org/10.1016/j.future.2021.05.019
A8. Yang G, Lv H, Zhang Z, Yang L, Deng J, You S, et al. Keep healthcare workers safe: application of teleoperated robot in isolation ward for COVID-19 prevention and control. Chin J Mech Eng 2020;33:47. https://doi.org/10.1186/s10033-020-00464-0
A9. Rose L, Yu L, Casey J, Cook A, Metaxa V, Pattison N, et al. Communication and virtual visiting for families of patients in intensive care during the COVID-19 pandemic: a UK National Survey. Ann Am Thorac Soc 2021;18(10):1685-92. https://doi.org/10.1513/AnnalsATS.202012-1500OC
A10. Fan EM, Ang SY, Phua GC, Chen Ee L, Wong KC, Tan FC, et al. Factors to consider in the use of vital signs wearables to minimize contact with stable COVID-19 patients: experience of its implementation during the pandemic. Front Digit Health 2021;3:639827. https://doi.org/10.3389/fdgth.2021.639827
A11. Lee D, Yoon SN. Application of artificial intelligence-based technologies in the healthcare industry: opportunities and challenges. Int J Environ Res Public Health 2021;18(1):271 https://doi.org/10.3390/ijerph18010271
A12. Diligent Robotics [Internet]. Austin (TX): Diligent Robotics Inc.; c2023 [cited at 2023 Jul 20]. Available from: https://diligentrobots.com/.
A13. Zicari RV, Brusseau J, Blomberg SN, Christensen HC, Coffee M, Ganapini MB, et al. On assessing trustworthy AI in healthcare. Machine learning as a supportive tool to recognize cardiac arrest in emergency calls. Front Hum Dynamics 2021;3:673104. https://doi.org/10.3389/fhumd.2021.673104
A14. Yin P, Yang L, Du S, Qu S, Jia B, Zhao N. The effect of mobile wearable waist assist robot on lower back pain during lifting and handling tasks. Mob Netw Appl 2021;26:988-96. https://doi.org/10.1007/s11036-020-01667-4
A15. Maffoni M, Torlaschi V, Pierobon A, Zanatta F, Grasso R, Bagliani S, et al. Video calls during the COVID-19 pandemic: a bridge for patients, families, and respiratory therapists. Fam Syst Health 2021;39(4):650-8. https://doi.org/10.1037/fsh0000661
A16. Skalidis I, Muller O, Fournier S. CardioVerse: The cardiovascular medicine in the era of Metaverse. Trends Cardiovasc Med 2022 May 11 [Epup]. https://doi.org/10.1016/j.tcm.2022.05.004
A17. Raje S, Reddy N, Jerbi H, Randhawa P, Tsaramirsis G, Shrivas NV, et al. Applications of healthcare robots in combating the COVID-19 pandemic. Appl Bionics Biomech 2021;2021:7099510. https://doi.org/10.1155/2021/7099510
A18. Sanfilippo F, La Via L, Schembari G, Tornitore F, Zuccaro G, Morgana A, et al. Implementation of video-calls between patients admitted to intensive care unit during the COVID-19 pandemic and their families: a pilot study of psychological effects. J Anesth Analg Crit Care 2022;2(1):38. https://doi.org/10.1186/s44158-022-00067-2
A19. Yun JM, Park HS. Perception of the patient safety risk factors and safety management by nurses in emergency service, hospitals. J Korean Acad Fundam Nurs 2014;21(4):380-91. https://doi.org/10.7739/jkafn.2014.21.4.380