I. Introduction
Nomophobia is the fear of not being able to use a mobile phone and/or the services it offers [1]. The prevalence of nomophobia ranges from 6% to 73% among various populations [2]. This prevalence is predicted to increase, becoming a major problem, due to the massive use of smartphones; likewise, the global coronavirus disease 2019 (COVID-19) pandemic has increased the time of use of these devices [3].
This problem occurs more frequently in adolescents and young adults [4], a population that corresponds to university students, who present a high prevalence of severe nomophobia [5]. The major problems of nomophobia in this population are poor academic performance and sleep disturbances [6], because nomophobia can be associated with anxiety, stress, dependence, low self-esteem, social problems, and fear, which is followed by feelings of frustration and obsessive thoughts, among others [7]. In addition, excessive cell phone use is associated with harmful effects on physical health such as repetitive motion injuries, pain in elbows, wrists, back, shoulders and thumb, index and middle fingers, as well as migraines and numbness due to constant mobile phone use [8,9]. Furthermore, a lack of confidence, low self-esteem, and lack of social skills when making social connections cause more dependence on mobile phones [10]. It should also be taken into account that demanding academic and personal lives make the use of these devices indispensable [10,11].
It is important to determine the prevalence of nomophobia, as it is a global problem. Systematic reviews of the prevalence of nomophobia have been carried out; however, they are limited in evaluating general populations, and none used uniform criteria to establish the prevalence of nomophobia [2,5]. Therefore, the aim of the present review was to synthesize previously reported data on the prevalence of nomophobia, as well as to establish its prevalence according to severity in university students.
II. Methods
We performed a systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines 2020 [12]. The study protocol was registered on PROSPERO (No. CRD42021230740).
1. Eligibility Criteria
Cross-sectional studies reporting the prevalence of nomophobia in undergraduate or postgraduate university students were included. Studies that assessed nomophobia with the 20-item Nomophobia Questionnaire (NMP-Q) tool developed by Yildirim and Correia [13] were considered. We chose this instrument as an inclusion criterion, since it is the most widely used validated scale [14] and divides nomophobia into absent (20 points), mild (21–60 points), moderate (61–100 points) and severe (101–120 points) [A1]. Studies with fewer than 30 participants, duplicate populations, clinical trials, case-control studies, case reports, editorials, commentaries, clinical practice guidelines, opinions, and reviews were excluded.
2. Literature Search and Study Selection
A systematic search was conducted in five databases: Web of Science/Core Collection, Scopus, PubMed, Embase and Ovid MEDLINE on March 16, 2021. No language or publication date restrictions were applied. The full search strategy for each database is available in Supplementary Table S1. We also screened the reference list of all included studies for additional eligible studies.
The identified references were exported to the Rayyan program [15] where duplicates were manually removed. Subsequently, two authors (KGT and SDCD) screened articles by titles and abstracts to identify potentially relevant articles for inclusion. Selected studies then underwent full-text screening (KGT and SDCD). These processes were conducted independently, and a third author (DRSM) resolved discrepancies by reaching a consensus for the final decision.
3. Data Extraction
Two authors (KGT and SDCD) independently extracted the following data of interest using a Microsoft Excel sheet: author, year of publication, country, sample size, setting (undergraduate, postgraduate), age, sex, major, cut-off points used in the scale, and the prevalence of nomophobia overall and by severity. A third author (DRSM) resolved any discrepancies.
4. Risk of Bias
Two authors (KGT and SDCD) independently assessed the methodological quality of prevalence studies using the Joanna Briggs Institute Critical Appraisal Tool [16]. A third author (DRSM) resolved discrepancies at this stage. This scale has nine items with possible answers of “yes,” “no,” and “unclear” if the study did not have enough data to reach a conclusion about the item. For the quality score of the study, 1 point was given if it complied with each item, and 0 if it did not comply or did not make the item clear. For the prevalence analysis according to the risk of bias, a total score of 0–3 was considered as indicating low methodological quality, 4–6 moderate quality, and 7–9 high quality.
5. Statistical Analyses
We calculated the pooled prevalence of nomophobia in university students, using a random-effects model, 95% confidence intervals (CIs) using the exact method with the Freeman-Tukey double-arcsine transformation to stabilize variance. Studies using standardized cut-off points for the NMP-Q scale were included in the meta-analysis. To assess heterogeneity and its sources, we used the Cochrane Q statistic and the I2 test, and we performed subgroup analyses according to country, sex, and major. We also performed a sensitivity analysis according to the risk of bias of the studies. We also assessed publication bias with the Egger test, considering p < 0.05 as indicating the presence of publication bias. The analyses were performed with Stata version 16.0 (StataCorp, College Station, TX, USA).
III. Results
1. Search Results
After removing duplicate records, we identified 230 studies through database searching. We reviewed 78 full-text studies and selected 24 after applying the inclusion criteria. We also identified four studies by checking the references of the included articles. We finally included 28 studies in the review (Figure 1). Reasons for the exclusion of the full-text articles reviewed are given in Supplementary Table S2.
2. Studies’ Characteristics
Twenty-eight studies with a total of 11,300 participants were chosen (Table 1, Appendix 1). With respect to countries, 15 studies were conducted in India [A2,A5–A8, A12,A13,A19–A21,A23–A25,A27,A28], six in Turkey [A3, A10,A11,A15,A17,A26], and one each in Oman [A9], the United States [A14], Pakistan [A4], Kuwait [A16], Saudi Arabia [A18], Indonesia [A22], and Germany [A1]. In terms of populations, the majority had a mean age between 19 to 22 years, and 23 included undergraduate university students [A1,A2–A6,A8,A10–A15,A17–A22,A24,A26–A28], one included graduate students [A23], and four were conducted in both populations [A7,A9,A16,A25].
The majority of studies evaluated students majoring in health-related professions (medicine, nursing, physiotherapy, dentistry, and pharmacy, among others) while six studies did not mention the majors evaluated [A4,A5,A9,A16,A25,A26].
Regarding cut-off points, most studies classified nomophobia into four groups (absent 20; mild 21–59; moderate 60–99; severe 100–120), three studies used statistical methods to divide nomophobia into present and absent [A21,A23,A26], one used cut-off points to classify participants into two groups (absent < 59; present 60–100) [A6], and one study did not specify this information [A15].
3. Prevalence of Nomophobia in University Students
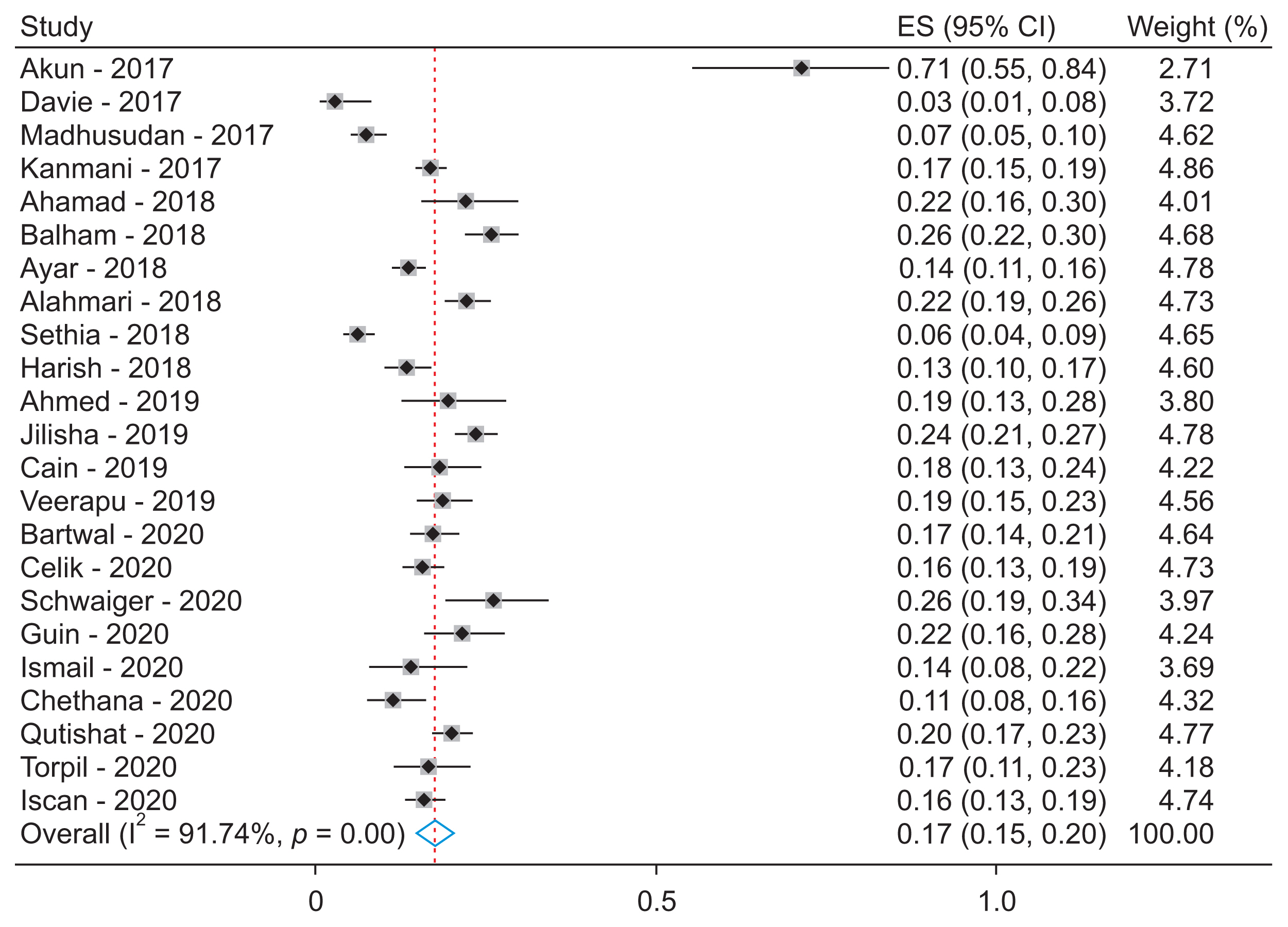
A meta-analysis was performed with the 23 studies that presented the prevalence of nomophobia in university students using standardized cut-off points to classify the condition as absent, mild, moderate, and severe [A1,A2–A5,A7–A14,A16–A20,A22,A24,A25,A27,A28]. The overall prevalence was close to 100%. According to severity, the prevalence of mild nomophobia was 24% (95% CI, 20%–28%; I2 = 95.3%), that of moderate nomophobia was 56% (95% CI, 53%–60%; I2 = 91.2%), and that of severe nomophobia was 17% (95% CI, 15%–20%; I2 = 91.7%). High heterogeneity was consistently evident in the meta-analysis (Figures 2–4).
In addition, the prevalence was assessed according to country, sex and major. Among the nine countries studied, Indonesia had the highest prevalence of severe nomophobia (71%; 95% CI, 55%–84%) and Germany had the lowest prevalence (3%; 95% CI, 1%–8%) [A1,A22]. In relation to major and sex, the prevalence was similar between categories, albeit with high heterogeneity (Table 2).
4. Risk of Bias
Regarding risk of bias, fewer than half of the studies met the items of “appropriate sampling frame,” “appropriate sampling,” “adequate sample size,” and “analysis conducted with sufficient sample coverage.” However, the majority met the items “validated methods for the identification of nomophobia,” “condition measured in a standard and reliable way for all participants,” and “appropriate statistical analysis” (Supplementary Table S3). When performing a sensitivity analysis according to risk of bias, we found that the prevalence rates among low-, moderate-, and high-quality studies were similar.
IV. Discussion
In the present study, we found that the overall prevalence of nomophobia in university students was approximately 100%. According to the severity of nomophobia, we found that one in four participants had mild nomophobia, more than half had moderate nomophobia, and approximately one in five participants had severe nomophobia. In addition, we evaluated the prevalence according to country, sex, and major; however, we found no differences between them.
Nomophobia is the fear of not having access to a mobile device or feeling disconnected [14]. We found two systematic reviews that assessed the prevalence of nomophobia. The first aimed to report on the prevalence of nomophobia and differences between sex and age; however, it did not perform a meta-analysis [2]. The second of these studies meta-analyzed the prevalence of nomophobia by population type, instrument, and severity [5]; however, the diagnostic criteria and severity classification used were not uniform. Therefore, we focused on evaluating the prevalence of nomophobia in university students, including studies that assess nomophobia with the NMP-Q scale. Furthermore, in the meta-analysis, we only included studies using standardized cut-off points for defining nomophobia as absent (20), mild (21–59), moderate (60–99), and severe (100–120). Regarding prevalence, the aforementioned systematic review found that the prevalence of severe nomophobia in university students was 25.5% (95% CI, 18.5%–34.0%; I2 = 97.0%) [5]. This overall prevalence is slightly higher than that found in the present study; however, the confidence intervals overlap. However, that study could not be compared regarding the other grades (mild and moderate) since it did not present the corresponding results.
When analyzing the prevalence rates according to major and sex, we found that they were similar. This last finding differs from the previous literature, where it was described that women were more likely to have nomophobia [2]. However, when evaluating prevalence rates by country, we found that most studies were from India, and the study that presented the highest prevalence of severe nomophobia was from Indonesia [A22].
In addition to the characteristics assessed, the prevalence of nomophobia and its severity can vary due to various factors.
The results of the research carried out highlight a high prevalence of moderate and severe nomophobia. The importance of nomophobia lies in the fact that it is associated with mental health problems, such as increased stress, anxiety, irritability, insomnia and depression, and can cause personality disorders and problems of self-esteem, loneliness or social isolation, and unhappiness [17]. It can also cause cognitive and motor impulsivity, whereby a person cannot concentrate on activities or performs them without thinking [6]. This can especially affect university students, in whom it has previously been reported that levels of nomophobia have a positive relationship with anxiety, stress and depression, and also interfere with their interpersonal relationships and academic performance, since a higher level of nomophobia was associated with worse academic performance [18]. It has even been proposed to include this phobia in the Diagnostic and Statistical Manual of Mental Disorders (DSM) fifth edition, due to its growing importance [19]. To address this problem, online educational interventions with interactive interfaces have been shown to decrease nomophobia; however, studies evaluating other types of interventions to address this problem are still lacking [2,19].
The included studies had limitations. We found high heterogeneity despite uniformity in the NMP-Q cut-off points used to classify nomophobia severity. Because five studies did not use standardized cut-off points to define nomophobia, they were excluded from the quantitative synthesis. This heterogeneity could be explained by differences in the sampling frame between the included studies. Only three articles conducted research at more than one university and in at least two majors. Furthermore, only six studies used random sampling or surveyed the entire population and only nine reported the sample calculation. Similarly, the diversity of majors and countries included in the meta-analysis would contribute to the high heterogeneity. Other factors that could explain the heterogeneity are the daily hours of phone use, social skills, and the year of study; however, these data are underreported in studies. Furthermore, worldwide, we found 26 studies from the Middle East and Asia that met the inclusion criteria, and only two studies in Europe and America.
It is recommended that future prevalence studies use random sampling, report the sample calculation, and detail the setting, specifying the major, year of study, age and sex of the participants. In addition, it is recommended that studies use the cut-off points of the NMP-Q scale to define nomophobia as absent, mild, moderate, and severe and that they present prevalence rates according to characteristics such as sex, major, and year of study. Finally, more studies are needed in other European and American countries.
Our study also has certain strengths. We conducted a comprehensive search of multiple databases and reviewed the references of included studies to capture more studies. In addition, we only included studies that used the NMP-Q scale to standardize and find studies with comparable prevalence rates. We also performed subgroup analyses to assess the heterogeneity found.
The prevalence of nomophobia in university students was very high. According to severity, the prevalence of mild, moderate, and severe nomophobia was 24%, 56%, and 17%, respectively. Regarding countries, Indonesia had the highest prevalence of severe nomophobia (71%) and Germany had the lowest (3%). The prevalence was similar according to sex and major. We recommend that further studies be conducted in more countries using the NMP-Q scale to make them comparable. We also suggest educational programs on the appropriate use of technology in university students.