Association between Health Information Technology and Case Mix Index
Article information
Abstract
Objectives
Health information technology (IT) can assist healthcare providers in ordering medication and adhering to guidelines while improving communication among providers and the quality of care. However, the relationship between health IT and Case Mix Index (CMI) has not been thoroughly investigated; therefore, this study aimed to clarify this relationship.
Methods
To examine the effect of health IT on CMI, a generalized estimation equation (GEE) was applied to two years of California hospital data.
Results
We found that IT was positively associated with CMI, indicating that increased IT adoption could lead to a higher CMI or billing though DRG up-coding. This implies that hospitals' revenue could increase around $40,000 by increasing IT investment by 10%.
Conclusions
The positive association between IT and CMI implies that IT adoption itself could lead to higher patient billings. Generally, a higher CMI in a hospital indicates that the hospital provides expensive services with higher coding and therefore receives more money from patients. Therefore, measures to prevent upcoding through IT systems should be implemented.
I. Introduction
Health information technology (IT) can assist providers in ordering medication and adhering to appropriate guidelines in the treatment of disease [1] while improving communication among providers within and between organizations [2]. Health IT is particularly useful for the gathering, organization and display of information, as well as facilitation of follow-up and other vital functions. [34]. Moreover, health IT could help improve the quality of care by reducing errors [567] and improving patient safety by preventing adverse drug events [8910].
Some studies have reported that health IT adoption is associated with reduced expenses in the hospital setting due to improved efficiency after health IT adoption [11]. However, the effect of health IT on healthcare costs still is not completely understood because health IT could be used by providers to increase billing (i.e., up-coding) [111213]. Recently, increasing concerns have emerged that the implementation of IT systems is likely to make it easier for providers to change patients' billing codes, and this could contribute to rising health expenditures. Some vendors explicitly advertise that their EMR will help physicians raise the level of billing codes. For example, one EMR vendor advertises on its website that its product will result in an increase of one coding level for each patient visit [1415]. This up-coding issue related to IT adoption could damage the national healthcare financial system. According to the US Office of Inspector General (OIG), the federal government recovered nearly $5.7 billion and $3.35 billion in healthcare fraud cases in 2014 and 2015, respectively.
Despite all of these concerns, few studies have investigated the relationship between IT system adoption and healthcare providers' revenue-enhancing practices. Li [12] and Ganju et al. [13] used the hospital-level Case Mix Index (CMI) as a payment measure and found that when hospitals adopted health IT systems including Electronic Medical Record (EMR) and computerized physician order entry (CPOE) functions, reimbursement was inflated through diagnosis-related group (DRG) up-coding. However, Adler-Milstein and Jha [14] did not find any significant relationship between IT adoption and billing. They used the DRG coding ratio as a payment measure based on patient level and found that payments per discharge were essentially the same for IT adopters and non-adopters. They concluded that the hospitals considered in their studies were not systematically using EHRs to increase reimbursement.
These previous studies used specific functions, namely, EMR and CPOE, as measures of IT, although there may be more than 50 health IT systems in a hospital [16]. Thus, it would be somewhat difficult to separate specific functions from others, which could result in unobserved variable problems. Therefore, in this study, health IT was measured as a continuous variable, not just as a dummy variable as in previous studies [121314]. Using a variable different from those used in previous studies, this study examined the effect of IT investment on the CMI by analyzing data obtained from the California Office of Statewide Health Planning and Development (OSHPD) from 2006 to 2007.
II. Methods
1. Data
We used hospital financial data obtained from the California OSHPD, as well as data from an American Hospital Association (AHA) survey and Healthcare Information and Management Systems Society (HIMSS) data. The California hospital financial data include patient utilization, hospital characteristics, and financial information. This data has been used in healthcare and economic studies [1718]. The AHA data provide detailed statewide hospital information, such as hospital staffing, profiles, and utilization. The HIMSS provides a variety of detailed historical data, reports, and white papers about IT use in hospitals and integrated healthcare delivery networks on more than 5,000 US hospitals and the ambulatory facilities associated with these hospitals. In this study, data from 200 hospitals were considered from a 2-year period from 2006 to 2007.
2. Dependent Variable
The dependent variable was the CMI, which is a relative value assigned to the DRG of patients in a medical care environment. It is applied to determine the resource allocation to take care of the patients in a group [18]. For the CMI, each patient treatment record is assigned a Medicare Severity-DRG (MS-DRG) based on the patient characteristics. An MS-DRG has a weight representing the national average hospital resource consumption per patient for that group, relative to that of all patients [19]. The CMI was used as a payment measure to examine the relationship between IT adoption and billing [121314].
3. Independent Variable
As the key explanatory variable, health IT expenditures were measured in dollar amounts, which were extracted from each hospital's trial balance worksheets and supplemental information sheets. IT expenditures include IT capital-related cost (i.e., physical capital, purchased services, lease/rental, and other direct expenditures) and IT labor-related cost (i.e., salaries and wages, employee benefits, and professional fees) [2021].
The OSHPD data did not provide the adoption status of specific IT systems, such as EMR, CPOE, etc. To assess the validity of our IT capital measure, we examined its relationship to the discrete measures of more than 50 health IT systems (i.e. EMR, CPOE, PACS, patient billing, order entry, radiology information management, clinical documentation, etc.) based on information provided by the HIMSS, and we found that the adoption of IT systems is associated with IT capital investment. Thus, this measure of IT expenditure included all of the IT systems mentioned above, not specific ones.
We controlled two groups of independent variables, including hospital/market characteristics and volume of hospital service. The hospital/market characteristics included ownership (for-profit, not-for-profit, and public), teaching status (being a Council of Teaching Hospitals and Health Systems member), network hospital status (system member), number of beds (five specialized bed types: adult general acute, pediatrics, obstetrics, cardiac intensive, and neonatal intensive) and competition, which was measured according to the Herfindahl-Hirschman Index (HHI) for each hospital based on admissions given the geographical market of the health service area [171820212223]. The values used to calculate volume included total admissions, outpatient visits, percentage of Medicare and Medicaid admissions out of total admissions, emergency room (ER) visits, and the numbers of inpatient and outpatient surgeries.
4. Statistical Analyses
To examine the effect of IT on CMI, this study utilized a generalized estimation equation (GEE) with log link and normal distribution. This estimation approach has been used in many studies focused on population-averaged effects [24]. For the covariance matrix, the independent variance model was adopted based on the smallest independence model criterion (QIC) [25]. The two groups of independent variables (hospital/market characteristics and volume) as well as IT expenditure were controlled. All analyses were conducted using Stata 11.2 software (StataCorp LLC., College Station, TX, USA).
III. Results
Table 1 shows the descriptive statistics for the variables used. The first row shows the CMI and IT investment. The average CMI was 1.106, but the standard deviation was a little low (0.256). Average IT investment was over 11 million. The second row of Table 1 shows the hospital characteristics. Not-for-profit hospitals accounted for almost 55% of the hospitals included in this study, while profit and public hospitals together accounted for 45%. Teaching and network hospitals accounted for 7.0% and 18.5%, respectively. Competition measured according to the HHI was 64.4%. The average number of specialized beds was 103 for adult general acute, 7 for pediatric general acute, 16 for obstetric, 5 for cardiac intensive, and 8 for neonatal intensive care. Network hospitals accounted for 18.8% of the hospitals considered.
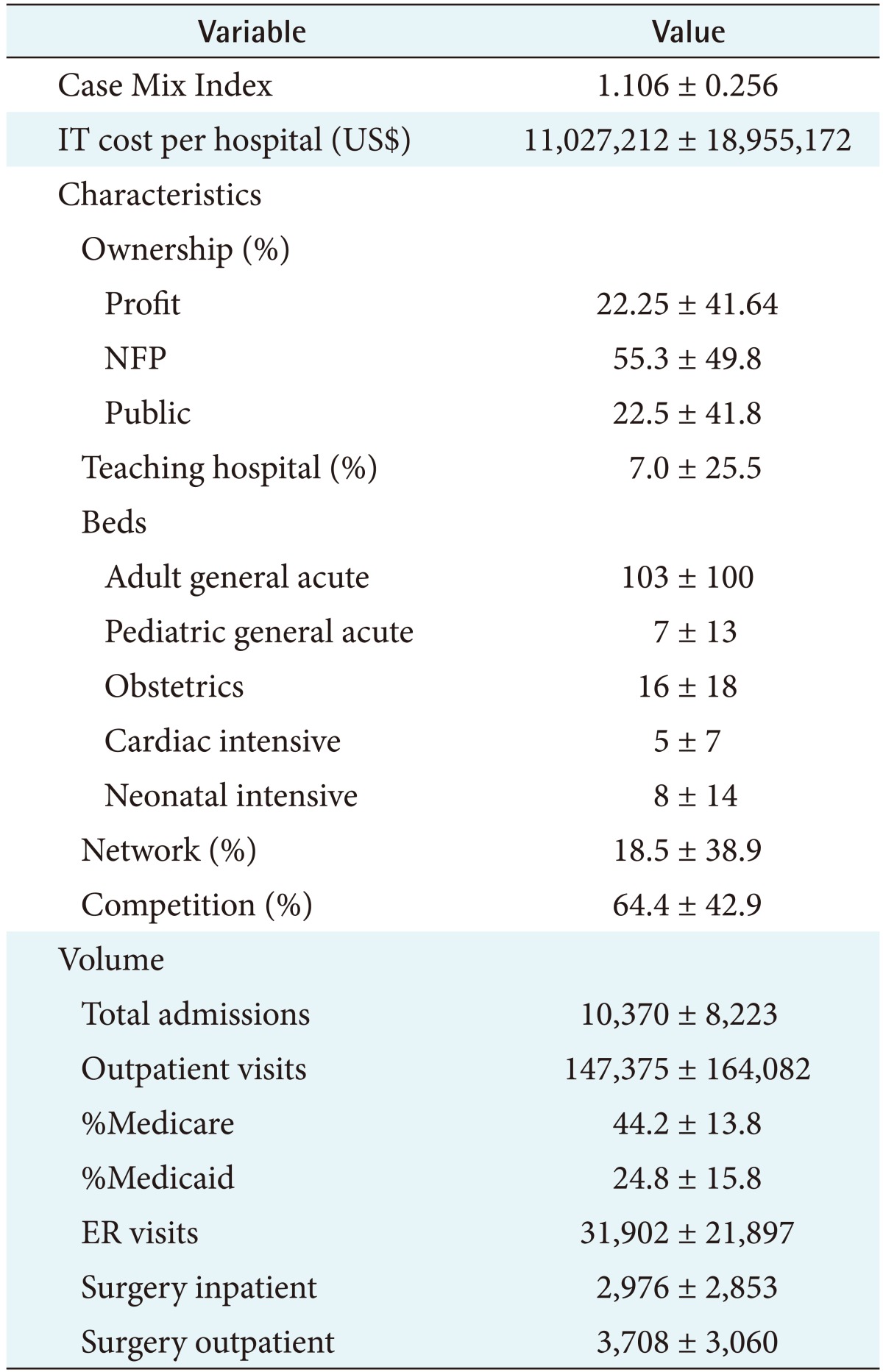
Descriptive statistics for California hospitals from 2006 to 2007
The last row of Table 1 shows hospital volume. There were 10,370 total admissions and 147,375 outpatient visits. The percentage of Medicare admissions out of total admissions was 44.1%, and the percentage of Medicaid admission out of total admissions was 24.8%. The total number of ER visits was 31,902. The numbers of surgery inpatient and outpatient operations were 2,976 and 3,708, respectively.
Table 2 shows the variations of the key variables such as CMI and IT cost between 2006 and 2007. The average CMI increased by 1.5% from 1.098 to 1.114, and the average IT cost increased by 14% from $10,241,705 to $11,812,718.

Case Mix Index and IT cost variation between 2006 and 2007
Table 3 shows the GEE regression results. We found that IT was positively associated with CMI. For example, the CMI increased by 0.86% when IT investment increased by 10%. Hospital characteristics were also important factors in explaining CMI. Not-for-profit and public hospitals had lower CMI values than for-profit hospitals. However, teaching hospitals had higher CMI values than non-teaching hospitals. Only neonatal intensive beds were positively associated with CMI, while obstetric beds were negatively associated with CMI. Moreover, higher competition was associated with higher CMI values. In general, volume had a positive effect on CMI. The percentage of Medicare admission out of total admissions, ER visits, and inpatient surgeries were positively associated with CMI. However, the percentage of Medicaid admission out of total admissions was negatively associated with CMI.

GEE regression results with log link and normal distribution for California hospitals from 2006 to 2007
IV. Discussion
This study examined the effect of health IT on CMI by considering hospital, market, and volume characteristics using data obtained from California hospitals during a two-year period. Unlike previous studies, we used continuous measurement of IT investment and found that IT was positively associated with CMI, indicating that increased IT adoption could lead to higher CMI values or higher billing though DRG up-coding.
Generally, a higher CMI in a hospital indicates that the hospital provides expensive services with higher coding and therefore receives more money from patients. Our results imply that hospitals could increase around $40,000 by increasing their IT investment by 10%, such an increase would represent a significant increase in profits for hospitals [26]. Our results are consistent with the findings of previous studies [1213], which also found that IT adoption led to inflated reimbursement through DRG up-coding. These results confirmed that patient coding can be easily manipulated by using IT systems.
Regarding ownership, for-profit hospitals had higher CMI values associated with IT in comparison to not-for-profit and public hospitals. This finding is also consistent with those of other studies. Generally, for-profit hospitals are keen to earn profits, which may result from a higher CMI [12]. Teaching hospitals had higher CMI values because teaching hospitals may serve as referral centers for patients with severe diseases [27].
Among the types of beds, only neonatal intensive beds were positively associated with CMI. A neonatal unit provides mechanical ventilation, neonatal surgery, and special care for the sickest infants born in a hospital or transferred from another institution [28]. Thus, more neonatal intensive beds may result in a higher CMI. Network hospitals had higher CMI values. These hospitals may have had tougher cases or better medical record systems [29].
Among the volume variables, the percentages of Medicare, ER visits, and surgery inpatients are positively associated with CMI. Medicare patients are those who are older than 65 and may have more severe or chronic diseases. ER visits involve emergency situations and may require more resources than regular visits. Inpatient surgeries also require more resource to treat patients.
The results of this study suggest that the inflation of billing codes through health IT systems has a major impact on the healthcare industry. First, inflated billing leads to medical payment increases, which may not be justified by clinical benefits. Moreover, it may undermine risk-adjusted quality measurement. Finally, up-coding could degrade data integrity and the quality of care.
This study has important policy implications. Policy makers, researchers, and health professionals should be cautious in interpreting the effects of health IT on CMI, and they should remember that IT adoption itself could lead to higher patient billing. Thus, measures to prevent up-coding through IT systems should be implemented. For example, EMR systems should be monitored and audited at the payer side, and the way vendors design their EMR products should be regulated.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.